
Riley
 Case Background
Case Background
Name: Riley
Age: 12 years old
Sex: Male, Castrated
Breed: Shih Tzu
Weight: 6 kg
Reason for visit: Presented two days ago to your colleague for a complaint of respiratory difficulty for one week. Now the owner, Mr. Brown, has brought him back to you because he has noticed a distended abdomen and is concerned because Riley is not eating well. During the initial visit a murmur was identified and Riley was tentatively diagnosed with CHF and started on Furosemide, enalapril and spironolactone.
Medications: Heartworm prevention: Heartgard® plus and Frontline®
Age: 12 years old
Sex: Male, Castrated
Breed: Shih Tzu
Weight: 6 kg
Reason for visit: Presented two days ago to your colleague for a complaint of respiratory difficulty for one week. Now the owner, Mr. Brown, has brought him back to you because he has noticed a distended abdomen and is concerned because Riley is not eating well. During the initial visit a murmur was identified and Riley was tentatively diagnosed with CHF and started on Furosemide, enalapril and spironolactone.
Medications: Heartworm prevention: Heartgard® plus and Frontline®
 Clinical History
Clinical History
Please review Riley’s clinical history.
Attitude/demeanor: Bright and alertCoughing: None reported
Respirations: Increased inspiratory effort with shallow breathing
Exercise intolerance: Has generally been slowing, but is now more reluctant to exercise
Sleep patterns: Sleeping well, but he prefers to sleep on his belly and not on his side
Weight change (loss or gain): Significant abdominal distension
Appetite: Not eating as well for the last 2 days
Usual diet: Science Diet® maintenance dry
Vomiting: None reported
Diarrhea: None reported
Syncope: None reported
Change in urinary habits: Increase in urinating since meds started yesterday
Change in drinking habits: Increase in drinking since meds started yesterday
Other symptoms or signs: None reported
 Physical Exam - General
Physical Exam - General
Please review the results of Riley’s physical exam.
Body condition: Good, BCS 6/9Attitude: Alert, somewhat anxious
Mobility | gait: Normal gait on inspection
Posture: Standing or sitting
Hydration: Normal
Body temperature: 100.3 F
Arterial pulse – rate, regularity, intensity: 132 beats/min, occasional premature beat, pulses fair
Respiratory rate & effort: 24 breaths per minute, normal
Mucous membranes – color & CRT: Normal color and CRT
Jugular venous pulse & pressure: Pulsations present to the level of the mandible bilaterally
Abdominal palpitation: Severe abdominal distension, fluid wave suspected, internal organs difficult to palpate
Lymph nodes: Normal
Oral cavity: Mild dental calculus
Other abnormalities: None
 Physical Exam - Auscultation
Physical Exam - Auscultation
Let’s auscult Riley’s heart & lungs. (Recommend high-end headphones)
The following recording is taken when the stethoscope is placed over the left apex. Similar sounds are heard when the stethoscope is placed over the right mid-heart.Listen to Riley's heart sounds
 Physical Exam ‑ Differential Diagnosis
Physical Exam ‑ Differential Diagnosis
The following are potential diagnosis for you to consider at this time. Based on the history and the physical examination, please indicate the likelihood of each as:
- High (could explain most or all of the signs)
- Possible (less likely to explain most of the signs)
- Unlikely
STAGE C MVD (MYXOMATOUS VALVULAR DEGENERATION)
STAGE C DCM
RIGHT SIDED CHF SECONDARY TO HEARTWORM DISEASE
PERICARDIAL EFFUSION CAUSING ASCITES (TAMPONADE)
Diagnostic Test Selection
Non-invasive blood pressure
CBC with platelet count
Serum biochemical profile (includes electrolytes)
Urinalysis
Serum thyroxine (T4)
Heartworm antigen test
Heartworm antibody test
NT-PROBNP
Thoracic radiographs
Abdominal radiographs
Echocardiogram with doppler studies
Abdominal ultrasound
ECG rhythm strip or 6 lead ECG
Ambulatory ECG - holter ECG or event monitor
 Blood Pressure
Blood Pressure
Systolic blood pressure: 110mmHg
Diastolic blood pressure: Not available for this case
Mean blood pressure: Not available for this case
Consensus Statements of the American College of Veterinary Internal Medicine (ACVIM) provides the veterinary community with up-to-date information on the pathophysiology, diagnosis, and treatment of clinically important animal diseases. In 2018, ACVIM published guidelines for the identification, evaluation, and management of systemic hypertension in dogs and cats in the the Journal of Veterinary Internal Medicine.
Click here to view and download a PDF of the ACVIM consensus statement, guidelines for the identification, evaluation, and management of systemic hypertension in dogs and cats.
Diastolic blood pressure: Not available for this case
Mean blood pressure: Not available for this case
Consensus Statements of the American College of Veterinary Internal Medicine (ACVIM) provides the veterinary community with up-to-date information on the pathophysiology, diagnosis, and treatment of clinically important animal diseases. In 2018, ACVIM published guidelines for the identification, evaluation, and management of systemic hypertension in dogs and cats in the the Journal of Veterinary Internal Medicine.
Click here to view and download a PDF of the ACVIM consensus statement, guidelines for the identification, evaluation, and management of systemic hypertension in dogs and cats.
 Radiography
Radiography
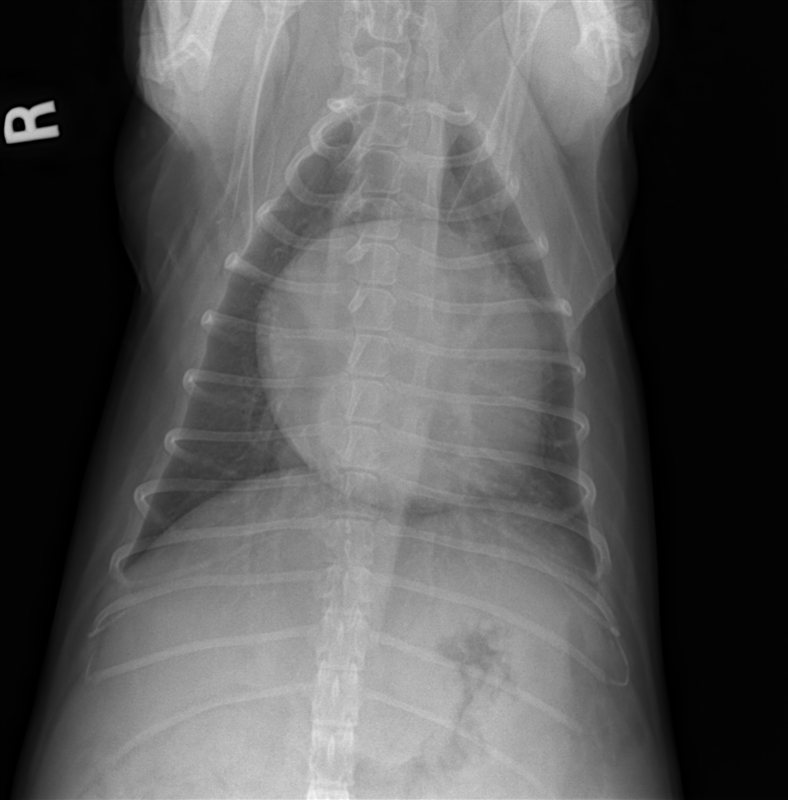
Please review Riley’s radiographs
Click here for Riley’s radiograph viewer (measure VHS and VLAS here) View the ventral dorsal radiograph
Riley's ventrodorsal view
Riley's right lateral view
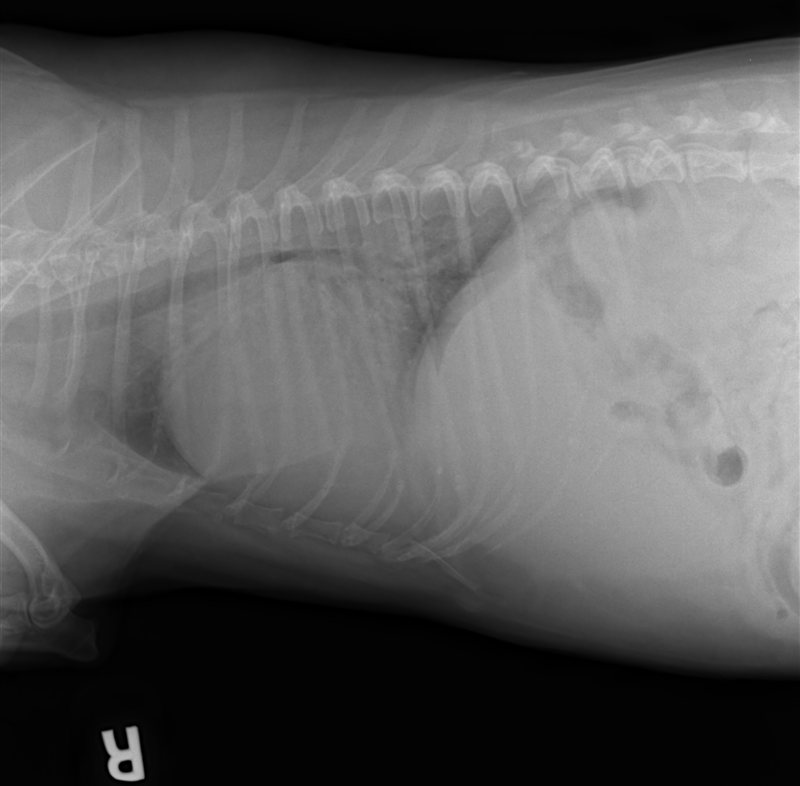
Is there evidence of pleural effusion or pulmonary edema to explain the respiratory signs?
Is Riley's heart enlarged?
 Clinical Labs
Clinical Labs
Please review Riley’s lab results
SERUM CHEMISTRIESBUN: 29 mg/dL, Normal: 6 – 25 mg/dL
Creatinine: 0.8 mg/dL, Normal: 0.5 – 1.6 mg/dL
Sodium: 145 mmol/L, Normal:139 – 154 mmol/L
Potassium: 4.5 mmol/L, Normal: 3.6 – 5.5 mmol/L
Chloride: 4.5 mmol/L, Normal: 3.6 – 5.5 mmol/L
ALT: 33 IU/L, Normal: 12 – 118 IU/L
ALP: 185 IU/L, Normal: 5 – 131 IU/LHEARTWORM
Heartworm test results: Negative within the last 6 monthsURINALYSIS
Urinalysis – USG: Not performed
Urinalysis – protein: Not performed
Urinalysis – biochemical: Not performed
Urinalysis – sediment evaluation: Not performedCBC
White blood cells: Not evaluated
Red blood cells: Not evaluated
Platelets: Not evaluated
 Echocardiography
Echocardiography
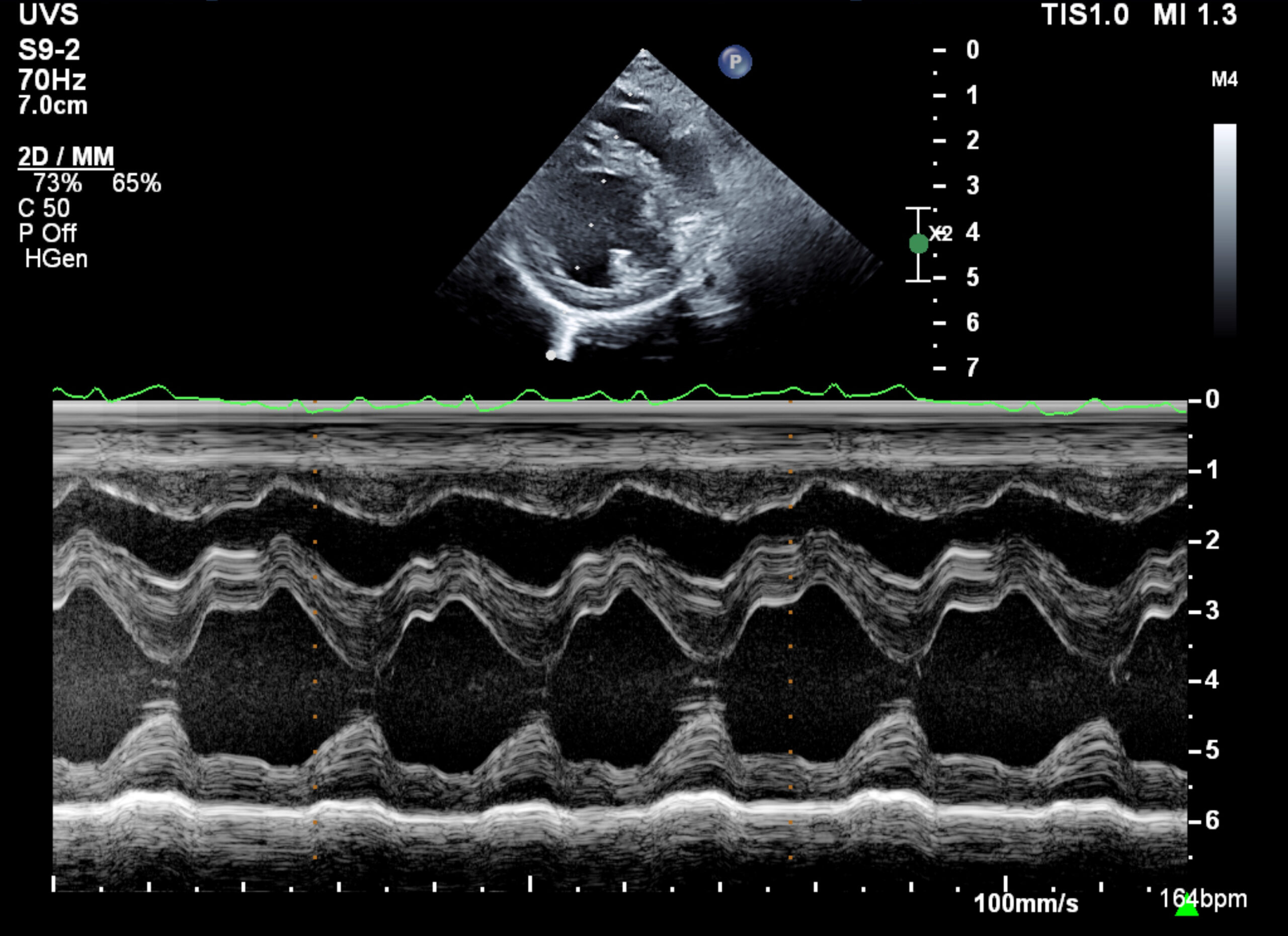
Please review the results of Riley’s echo. The images and videos were obtained by a cardiologist.
Subjective – lesions of valves, myocardium, pericardial space: No pericardial effusion; thickened mitral leafletsLV chamber size and thickness:Mild left ventricular enlargement
Left atrial size: Moderate to severe dilation
LVIDd & LVIDs: Diastole (3.22 cm); Systole (1.41 cm)
LV shortening fraction: Normal to hyperdynamic ~ 56%
RA, RV and pulmonary artery: Moderate right atrial and ventricular enlargement, moderately dilated main pulmonary artery
Effusions: Moderate ascites seen
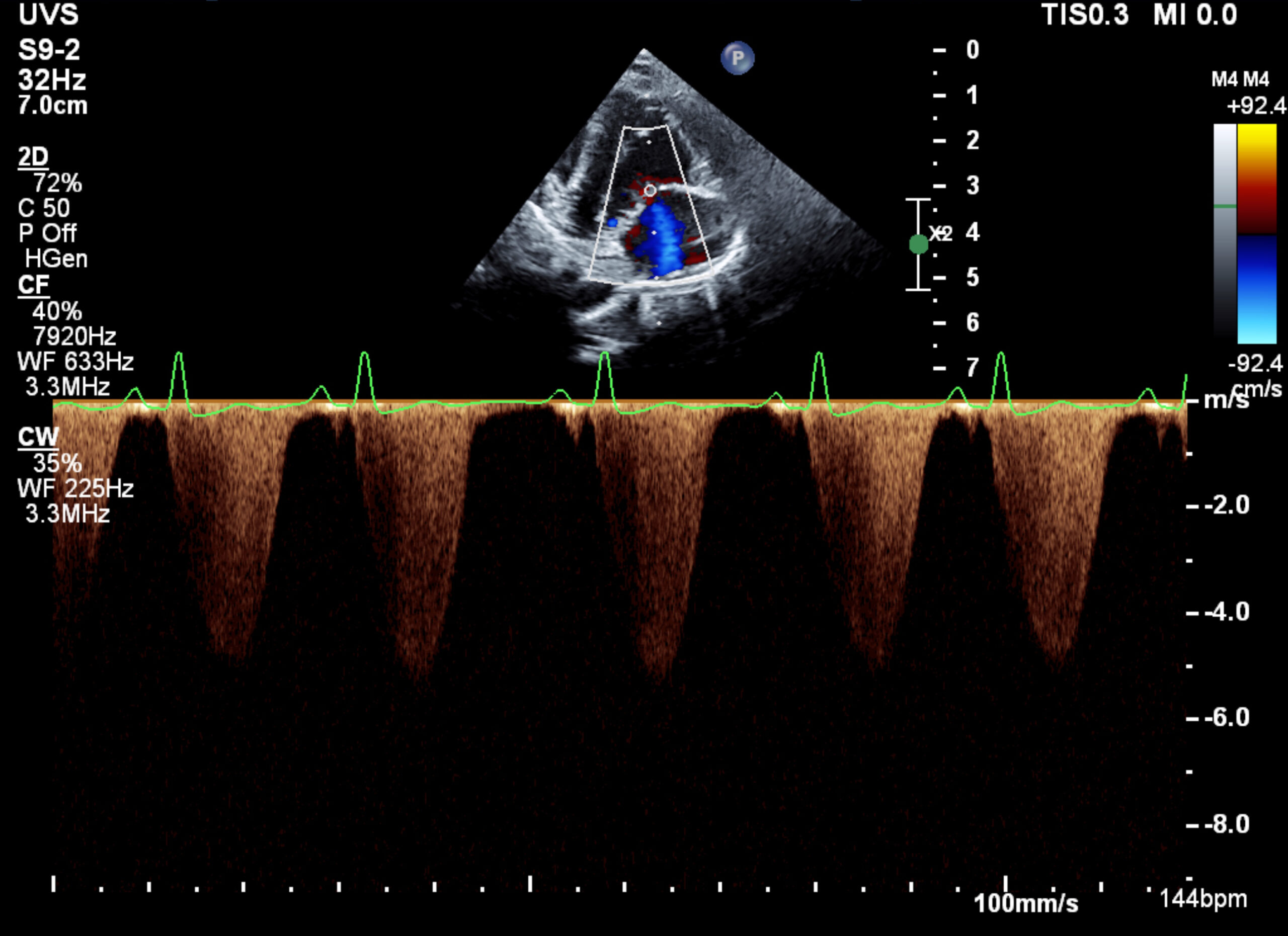
Doppler results: Mitral and tricuspid regurgitation; velocity of MR predicts normal systemic pressures; increased velocity of TR (~5.2 m/s) predicts severe pulmonary artery hypertension (~110 mmHg)Click here to view an M-mode of Riley's LV and RV
Riley's LV Echo
Riley Tricuspid Regurgitation Velocity
 Referral
Referral
Under most circumstances, the identification of severe pulmonary hypertension as a cause for right sided congestive heart failure would require a referral to obtain the echocardiographic imaging found in this case.
 Diagnosis & Treatment
Diagnosis & Treatment
With the information obtained from the diagnostic testing above, please choose a diagnosis and treatment plan for Riley.
What is Riley’s cardiac diagnosis?
What treatments are recommended for Riley? Riley’s weight is 6kg
 Post Test - CE
Post Test - CE
To qualify for CE credit, please answer the following 5 questions.
Which of the following findings defines Riley as being in congestive heart failure?
Which of the following drug effects makes sildenafil useful in the treatment of this case?
The diagnosis of pulmonary hypertension is best evaluated on echo by interrogations of what flow?
Which of the following conditions best explains the cause of Riley’s pulmonary hypertension?
The presence of pulmonary hypertension can cause what clinical signs?
 RACE Certification
RACE Certification
RACE Certification
Fill out the following form in order to receive your certificate.