
Jasmine
 Case Background
Case Background
Name: Jasmine
Age: 12 years
Sex: Female, spayed
Breed: Shih Tzu
Age: 12 years
Sex: Female, spayed
Breed: Shih Tzu
 Clinical History
Clinical History
Please review Jasmine’s clinical history.
Coughing for the past 4-6 weeks; getting worse in the last week. A grade 4/6 systolic heart murmur was detected, loudest at the left apex of the heart. Jasmine has had no respiratory difficulty. Still has good energy and will go for walks. Eating and drinking fine.
 Radiographs
Radiographs
View Jasmine's right lateral radiograph
 View Jasmine's ventrodorsal radiograph
View Jasmine's ventrodorsal radiograph
Jasmine's right lateral radiograph
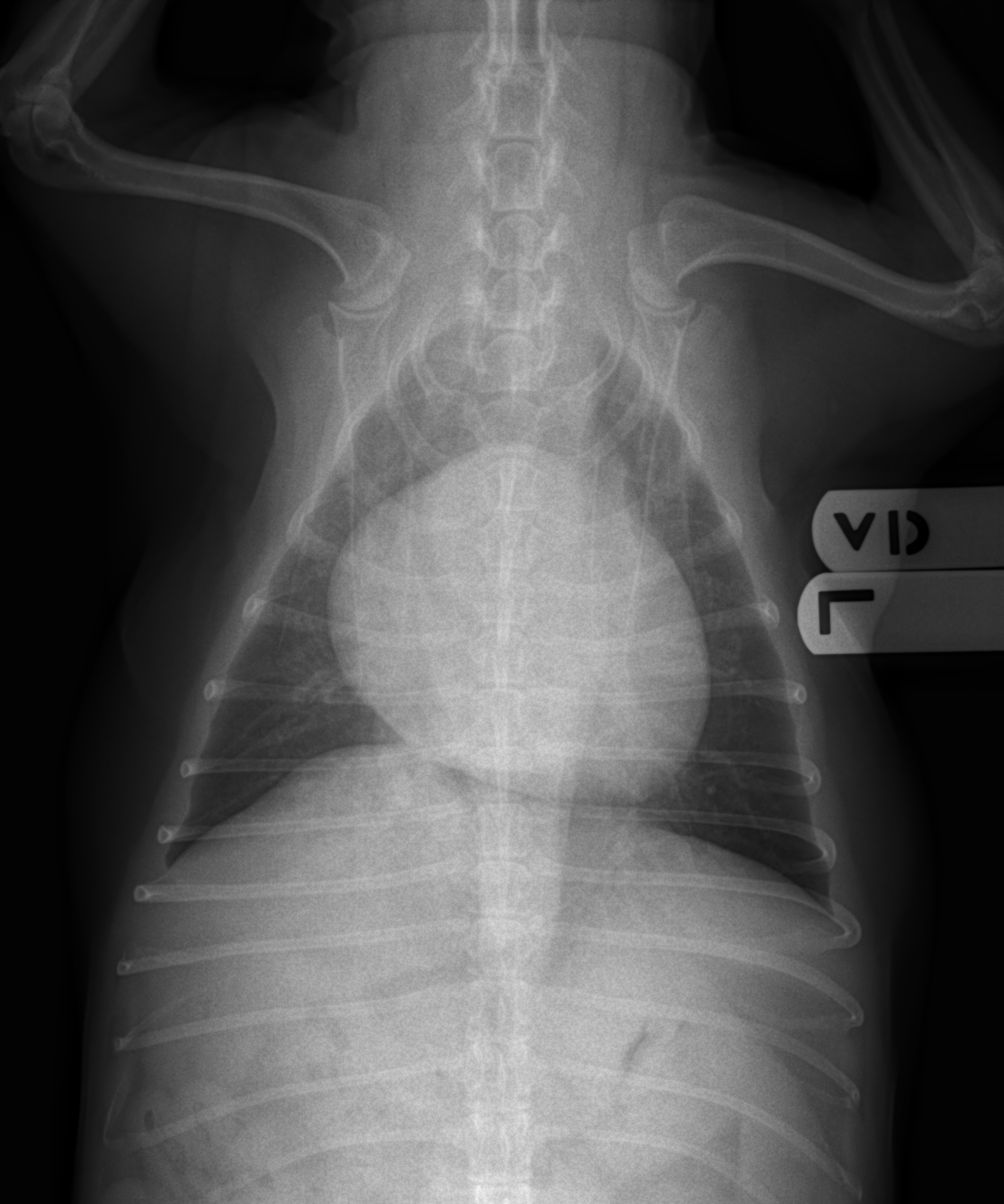
Jasmine's ventrodorsal radiograph
Technical details
Location of images: Thoracic radiographs obtained.
Views of images: Right lateral and ventrodorsal radiographs were obtained.Radiographic findings
Technical issues: May be slightly expiratory on lateral, increasing the subjective impression of the opacity of the pulmonary parenchyma in the perihilar area.
Cardiac size including VHS: VHS 11.5, predominantly LV and LA enlargement (especially on lateral, to a lesser extent on the VD); the VLAS is 3, consistent with left atrial enlargement. Subjectively, the right sided structures may also be enlarged (wide on lateral and VD suggests some RVE).
Other findings: Pulmonary vasculature relatively normal with no interstitial changes; no pleural effusion; patient is overweight; trachea narrows slightly, with significant narrowing of airways at heart base.
 Diagnosis & Treatment
Diagnosis & Treatment
Radiographic interpretation: Cardiac enlargement, predominantly left sided; pronounced left atrial enlargement associated with airway compression; no CHF. This patient’s signalment and physical findings of a left apical heart murmur are consistent with mitral regurgitation (likely due to myxomatous mitral valve disease). Based on her radiographic findings (including VHS and VLAS), she is in Stage B2.
Discussion: This patient has clear evidence for left sided enlargement, especially left atrial enlargement. The lack of any interstitial or vascular abnormalities suggests that the coughing is not a manifestation of congestive heart failure. Rather airway compression (with the potential for concurrent airway collapse) is the more likely explanation for the cough. This would fit with the otherwise normal presentation.
Treatment/management: The lack of congestive heart failure makes therapy with diuretics unnecessary. If mitral regurgitation and Stage B2 status is confirmed by echocardiography, therapy with pimobendan is indicated. Cough suppressants would be beneficial in this case given the presenting complaint, especially in the absence of concurrent pneumonia, edema or other pulmonary infiltrate. The use of ACE inhibitors can also be considered given the degree of cardiac enlargement and associated clinical signs.
Discussion: This patient has clear evidence for left sided enlargement, especially left atrial enlargement. The lack of any interstitial or vascular abnormalities suggests that the coughing is not a manifestation of congestive heart failure. Rather airway compression (with the potential for concurrent airway collapse) is the more likely explanation for the cough. This would fit with the otherwise normal presentation.
Treatment/management: The lack of congestive heart failure makes therapy with diuretics unnecessary. If mitral regurgitation and Stage B2 status is confirmed by echocardiography, therapy with pimobendan is indicated. Cough suppressants would be beneficial in this case given the presenting complaint, especially in the absence of concurrent pneumonia, edema or other pulmonary infiltrate. The use of ACE inhibitors can also be considered given the degree of cardiac enlargement and associated clinical signs.