
Queeny
 Case Background
Case Background
Name: Queeny
Age: 6 years
Sex: Female, spayed
Breed: Feline, domestic short hair
Age: 6 years
Sex: Female, spayed
Breed: Feline, domestic short hair
 Clinical History
Clinical History
Please review Queeny’s clinical history.
Patient presented for frequent coughing and wheezing. Patient has a history of chronic cough as well as severe, recurrent skin and ear infections suspected to be secondary to allergies. On examination the cat had a slightly increased expiratory effort but no distress; no murmurs or gallop sounds were evident.
 Radiographs
Radiographs
View Queeny's left lateral radiograph
 View Queeny's ventrodorsal radiograph
View Queeny's ventrodorsal radiograph

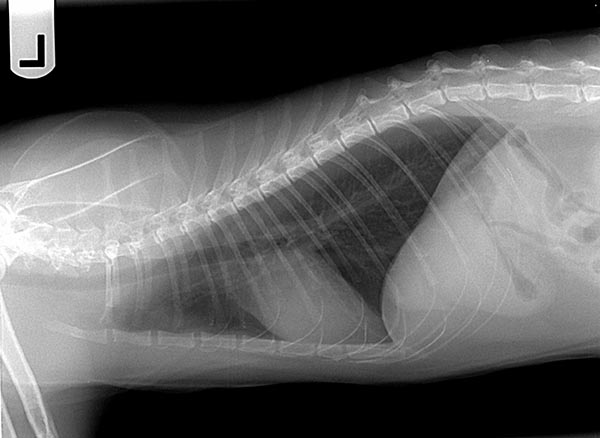
Queeny's left lateral radiograph
Queeny's ventrodorsal radiograph
Click here to view Queeny’s radiographic viewer (measure VHS)
Technical details
Location of images: Thoracic radiographs obtained.
Views of images: Left lateral and ventrodorsal throracic radiographs.Radiographic Findings
Technical issues: None.
Cardiac size including VHS: VHS 7.2. Cardiac silhouette appear mildly elongated, but this is suspected to be fat in the pericardiacophrenic ligament. There is also an opacity at the cranial base of the heart that is most commonly the ascending aorta/aortic arch, but can be the right auricle or pulmonary artery. Cardiac silhouette appears to have a normal size, except for a opacified bulge near the right atrium. This is generally a difficult area to interpret, as this could be adipose tissue, but given the mildly dilated pulmonary arteries, right atrial dilation must be a consideration. No pulmonary venous congestion, but the pulmonary artery to the cranial lung field (lateral) and to the right caudal lung field (VD) appear mildly distended.Pulmonary infiltrate distribute predominately perihilar and caudodorsal. Pulmonary infiltrate pattern, bronchial. No pleural effusion.
Other findings: None.
 Diagnosis & Treatment
Diagnosis & Treatment
Radiographic interpretation: Mild right atrial enlargement with mildly distended pulmonary arteries consistent with pulmonary hypertension. There is also a bronchial pattern consistent with feline asthma.
Discussion: These films are most consistent with feline asthma and secondary pulmonary hypertension. The history already suggests asthma in an allergy prone cat, so the presence of a bronchial pattern in the absence of any significant interstitial or alveolar infiltrate, strongly suggests feline asthma. Suspicion of pulmonary hypertension would also be high in a patient with chronic respiratory symptoms. An echocardiogram would be needed to confirm pulmonary hypertension.
Treatment/management: Patient was placed on a 3 week tapering dose of prednisolone 2.5mg every 12 hours. An albuterol metered dose inhaler was prescribed with an Aerokat(r) feline aerosol chamber if needed for asthmatic attacks leading to severe coughing or wheezing. Inasmuch as airway inflammation underlies asthma, the need for long-term anti-inflammatory therapy was discussed including using inhaled fluticasone if there is a good response to oral prednisolone. Clients were advised to view Youtube(r) videos regarding use of an inhaler. The medication costs associated with inhaled fluticasone were also mentioned, as this can be a practical factor affecting the acceptance of that treatment.
Discussion: These films are most consistent with feline asthma and secondary pulmonary hypertension. The history already suggests asthma in an allergy prone cat, so the presence of a bronchial pattern in the absence of any significant interstitial or alveolar infiltrate, strongly suggests feline asthma. Suspicion of pulmonary hypertension would also be high in a patient with chronic respiratory symptoms. An echocardiogram would be needed to confirm pulmonary hypertension.
Treatment/management: Patient was placed on a 3 week tapering dose of prednisolone 2.5mg every 12 hours. An albuterol metered dose inhaler was prescribed with an Aerokat(r) feline aerosol chamber if needed for asthmatic attacks leading to severe coughing or wheezing. Inasmuch as airway inflammation underlies asthma, the need for long-term anti-inflammatory therapy was discussed including using inhaled fluticasone if there is a good response to oral prednisolone. Clients were advised to view Youtube(r) videos regarding use of an inhaler. The medication costs associated with inhaled fluticasone were also mentioned, as this can be a practical factor affecting the acceptance of that treatment.