
Arco
 Case Background
Case Background
Name: Arco
Age: 10 years
Sex: Male
Breed: Male German Shorthaired Pointer
Weight: 32 kg
Reason for visit: Heart murmur detected prior to anesthesia for neutering due to history of prostatitis and prostatic hypertrophy (intact male). Arco is negative for heartworm disease based on a yearly antigen test and year-round monthly preventative.
Medications: None
Age: 10 years
Sex: Male
Breed: Male German Shorthaired Pointer
Weight: 32 kg
Reason for visit: Heart murmur detected prior to anesthesia for neutering due to history of prostatitis and prostatic hypertrophy (intact male). Arco is negative for heartworm disease based on a yearly antigen test and year-round monthly preventative.
Medications: None
 Clinical History
Clinical History
Attitude/demeanor: Quiet, alert and appropriate to surroundings
Coughing: None
Abnormal respirations: None
Exercise intolerance: None
Sleep patterns: No changes, normal
Weight change (loss or gain): None
Appetite: Has become somewhat more picky in past 6 months
Vomiting: One episode 3 days before presentation
Diarrhea: No
Syncope: No
Change in urinary habits: Some straining to urinate noted by owners, resulted in suspicion of prostatic disease
Change in drinking habits: Mildly increased water consumption in past year
Coughing: None
Abnormal respirations: None
Exercise intolerance: None
Sleep patterns: No changes, normal
Weight change (loss or gain): None
Appetite: Has become somewhat more picky in past 6 months
Vomiting: One episode 3 days before presentation
Diarrhea: No
Syncope: No
Change in urinary habits: Some straining to urinate noted by owners, resulted in suspicion of prostatic disease
Change in drinking habits: Mildly increased water consumption in past year
 Physical Exam - General
Physical Exam - General
Body condition: Lean, BCS 4/9
Attitude: Quiet and alert, slightly anxious
Mobility | gait: Normal
Posture: Normal
Hydration: Adequate, based on mucous membrane examination and normal capillary refill time
Body temperature: 101.2° F
Arterial pulse – rate, regularity, intensity: Strong pulses, no deficits
Rate & respiratory effort: 36 per minute, eupneic
Mucous membranes – color & CRT: Pale pink, moist
Jugular venous pulse & pressure: No jugular distention noted
Abdominal palpatation: Mildly tense, non-painful, no organomegaly or mass lesions identified
Lymph nodes: Peripheral lymph nodes symmetric, normal in size and texture
Oral cavity: Moderate dental tartar
Other abnormalities: Rectal exam revealed that prostate gland was out of reach of digital examination, no evidence of pain during exam
Attitude: Quiet and alert, slightly anxious
Mobility | gait: Normal
Posture: Normal
Hydration: Adequate, based on mucous membrane examination and normal capillary refill time
Body temperature: 101.2° F
Arterial pulse – rate, regularity, intensity: Strong pulses, no deficits
Rate & respiratory effort: 36 per minute, eupneic
Mucous membranes – color & CRT: Pale pink, moist
Jugular venous pulse & pressure: No jugular distention noted
Abdominal palpatation: Mildly tense, non-painful, no organomegaly or mass lesions identified
Lymph nodes: Peripheral lymph nodes symmetric, normal in size and texture
Oral cavity: Moderate dental tartar
Other abnormalities: Rectal exam revealed that prostate gland was out of reach of digital examination, no evidence of pain during exam
 Physical Exam - Auscultation
Physical Exam - Auscultation
Listen to Arco’s heart (Recommend high-end headphones)
Heart murmur intensity is usually graded on a scale of 1-6, where grades 5 & 6/6 are very loud murmurs with a precordial thrill (a palpable buzzing sensation on the thorax). Arco's thoracic palpation reveals no precordial thrill. This indicates that the heart murmur is likely to be graded as:
Careful auscultation allows localization of the heart murmur to the left cardiac apex. What is the timing of the murmur?
 Physical Exam - Differential Diagnosis
Physical Exam - Differential Diagnosis
The following are potential diagnosis for you to consider at this time. Based on the history and the physical examination, please indicate the likelihood of each as:
- High (could explain most or all of the signs)
- Possible (less likely to explain most of the signs)
- Unlikely
Myxomatous mitral valve disease with mitral regurgitation
Aortic stenosis or subaortic stenosis, previously undetected
Vegetative endocarditis of the mitral valve
Vegetative endocarditis of the aortic valve
Diagnostic Test Selection
Non-invasive blood pressure
CBC with platelet count
Urinalysis
Serum thyroxine (T4)
NT-ProBNP
Cardiac troponin-I
Blood culture
Thoracic radiographs
Abdominal radiographs
Echocardiogram doppler studies
Abdominal ultrasound
ECG rhythm strip or 6 lead ECG
 Radiography
Radiography
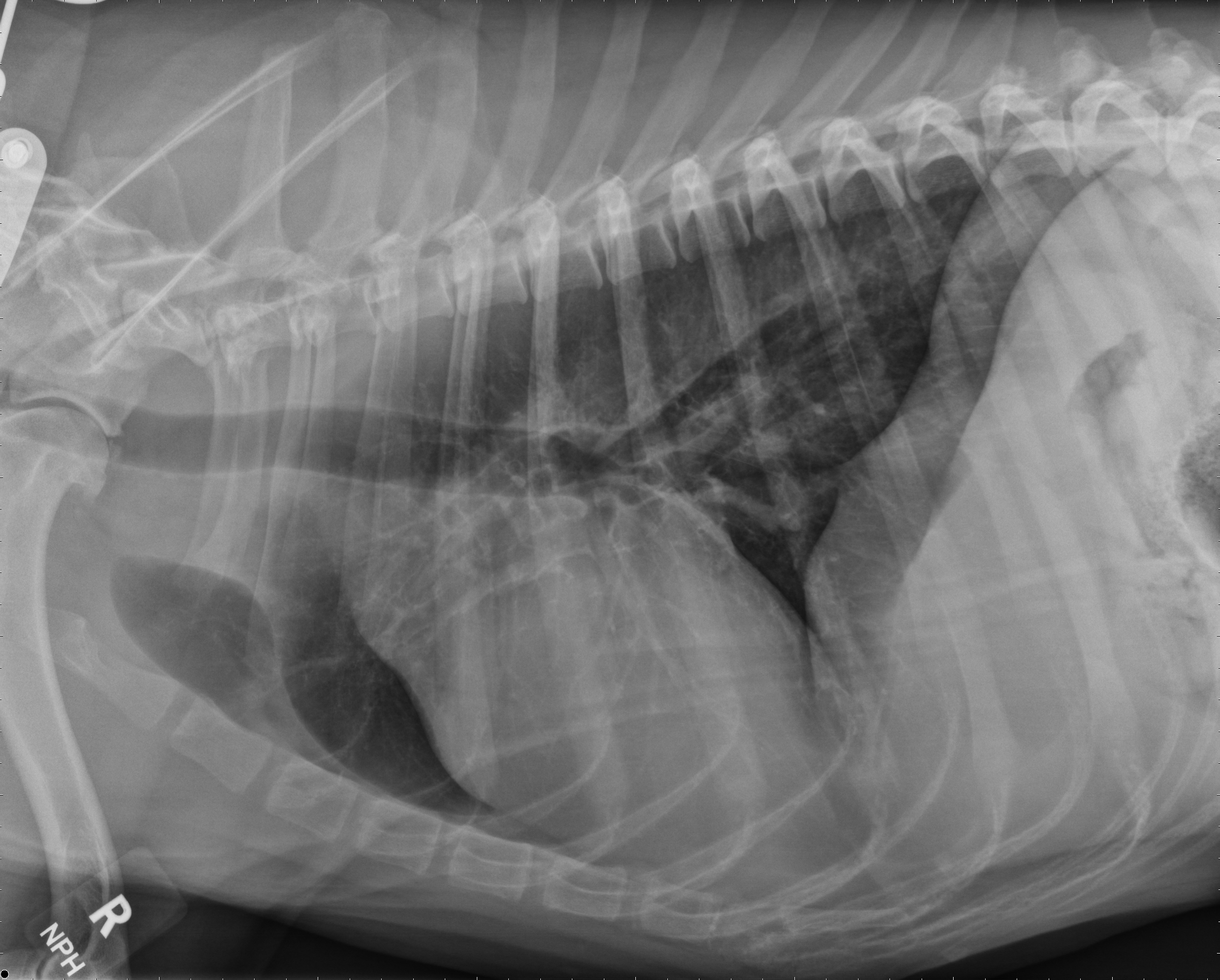
Please review Arco’s radiographs
Click here for Arco’s radiograph viewer (measure VHS and VLAS here) View the right lateral radiographArco's right lateral radiograph
Arco's ventral dorsal radiograph
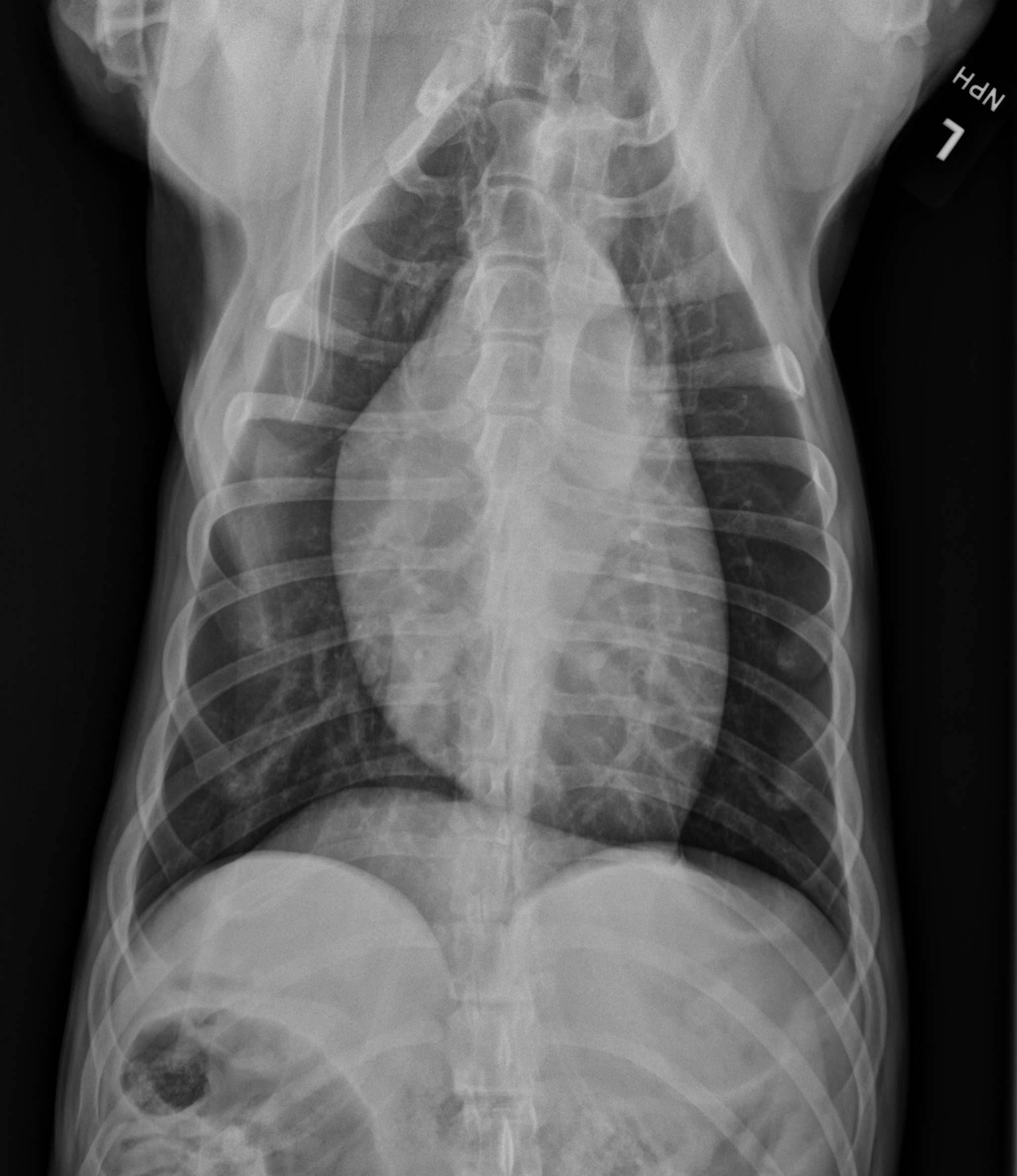
What is the vertebral heart size?
Which cardiac chambers/structures appear to be enlarged?
 Clinical Labs
Clinical Labs
Serum chemistries
BUN: 113 mg/dL Normal: 7-32 mg/dLCreatinine: 7.1 mg/dL Normal: 0.5 – 1.5 mg/dL
Sodium: 150 mm0l/L Normal:141 – 150 mm0l/L
Potassium: 3.9 mm0l/L Normal: 3.9 – 5.3 mm0l/L
Chloride: 121 mm0l/L Normal: 109 – 119 mm0l/L
ALT: 37 IU/L Normal: 14 – 87 IU/L
ALP: 47 IU/L Normal: 20 – 157 IU/L
Urinalysis
Urinalysis – USG: 1.012Urinalysis – protein: 3
Urinalysis – biochemical: Not Done
Urinalysis – sediment evaluation: RBCs: 5-10/hpf, WBC: rare, casts: none, crystals: few amorphous
CBC
White blood cells: 9.0 x 10^3/uL (5-14 x 10^3/uL)Red blood cells: Hct 39% (39-57%)
Platelets: 283 x 10^3/uL (175-500 x 10^3/uL)
 Echocardiography
Echocardiography
Please review Arco’s echocardiogram results
Subjective – lesions of valves, myocardium, pericardial space: 1. The mitral valve leaflets are mildly thickened. There are several jets of mitral regurgitation noted; overall severity appears to be mild to moderate. 2. The aortic valve is structurally normal. There is no evidence of aortic or subaortic stenosis. Mild to moderate aortic regurgitation is present. 3. The tricuspid valve is normal and there is no tricuspid regurgitation. 4. The pulmonary valve is normal. There is no evidence of pulmonic stenosis or pulmonic regurgitation.
LV chamber size & thickness: The left ventricle is severely thickened, globally. The LV diameter in diastole is normal compared to weight-based references. Both the LV wall and the interventricular septum are severely thickened compared to weight-based reference ranges.
Left atrial size: Left atrial diameter is normal subjectively. LA: Ao ratio is normal (1.11).
LVIDd & LVIDs: Both within normal reference ranges.
LV shortening fraction: 37%
RA, RV & pulmonary artery: All within expected size ranges.
Effusions: None
Doppler results: Aortic systolic velocity: 1.59 m/s, gradient ~10 mmHg (normal). Pulmonic systolic velocity: 0.87 m/s, gradient ~3 mmHg (normal).
 ECG
ECG
Click here for Arco's ECG
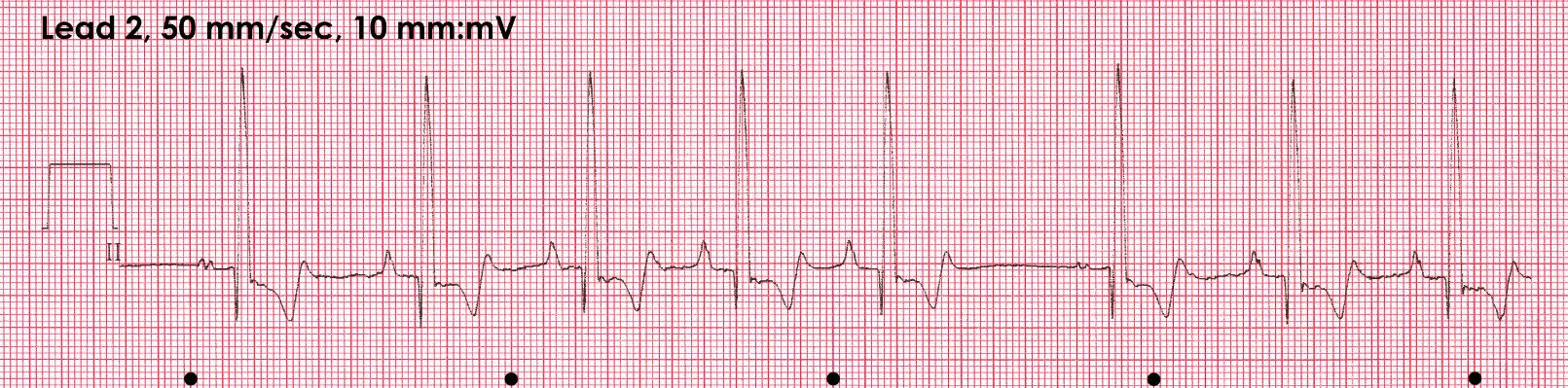 Technical quality, leads, paper speed, calibrations: Good quality recording, lead 2 rhythm strip, 50 mm/sec, 10 mm/mV
Technical quality, leads, paper speed, calibrations: Good quality recording, lead 2 rhythm strip, 50 mm/sec, 10 mm/mV
Artifacts: None
Rhythm- regular or irregular/ patterns: Irregular rhythm
P Wave abnormalities- morphology, amplitude, duration: P wave height and width are normal. Some P waves are notched. There is variable P wave morphology (complexes 1 and 6)
QRS abnormalities- axis, morphology, amplitude, duration: QRS height and width are normal
Abnormal intervals- PR, QRS, QT: All intervals are within reference ranges
Other: The T wave is biphasic
Arco's ECG
Artifacts: None
Rhythm- regular or irregular/ patterns: Irregular rhythm
P Wave abnormalities- morphology, amplitude, duration: P wave height and width are normal. Some P waves are notched. There is variable P wave morphology (complexes 1 and 6)
QRS abnormalities- axis, morphology, amplitude, duration: QRS height and width are normal
Abnormal intervals- PR, QRS, QT: All intervals are within reference ranges
Other: The T wave is biphasic
What is the heart rate and rhythm diagnosis? (black dots mark 1 sec. Intervals)
What is the likely cause of the variable p wave morphology noted here?
Summary of Current Test Results
Based on Arco’s laboratory assessment, severe azotemia with isosthenuria and proteinuria is present, making renal dysfunction likely. The urine sediment reveals proteinuria with an inactive sediment, making urinary tract infection less likely, but does not rule infection out completely. Arco’s echocardiographic findings combined with his radiographic findings indicate the presence of ACVIM Stage B1 mitral regurgitation, likely secondary to myxomatous valve disease. These findings are consistent with Arco’s age and breed. Severe left ventricular hypertrophy and aortic regurgitation without evidence of aortic/subaortic stenosis are suggestive of systemic hypertension. Protein-losing renal disease (glomerular disease) is common in older dogs and often associated with systemic hypertension. Additional diagnostic testing is indicated.
Additional Diagnostic Selection
Which of the following additional diagnostic tests are indicated for Arco?
Non-invasive blood pressure
Ocular/retinal examination
Coagulation profile
Urine protein: creatinine ratio
Serum thyroxine (T4)
Heartworm antigen test
Blood culture
Urine culture
Serology for tick-borne disease
Abdominal radiographs
Abdominal ultrasound
 Blood Pressure Results
Blood Pressure Results
Systolic blood pressure: 254 mmHg
Diastolic blood pressure: 138 mmHg
Mean blood pressure: 190 mmHg
Consensus Statements of the American College of Veterinary Internal Medicine (ACVIM) provide the veterinary community with up-to-date information on the pathophysiology, diagnosis, and treatment of clinically important animal diseases. In 2018, ACVIM updated guidelines for the identification, evaluation, and management of systemic hypertension in dogs and cats in the the Journal of Veterinary Internal Medicine. Click here to view and download a PDF of the ACVIM consensus statement, guidelines for the identification, evaluation, and management of systemic hypertension in dogs and cats.
Diastolic blood pressure: 138 mmHg
Mean blood pressure: 190 mmHg
Consensus Statements of the American College of Veterinary Internal Medicine (ACVIM) provide the veterinary community with up-to-date information on the pathophysiology, diagnosis, and treatment of clinically important animal diseases. In 2018, ACVIM updated guidelines for the identification, evaluation, and management of systemic hypertension in dogs and cats in the the Journal of Veterinary Internal Medicine. Click here to view and download a PDF of the ACVIM consensus statement, guidelines for the identification, evaluation, and management of systemic hypertension in dogs and cats.
What is your assessment of Arco's blood pressure results?
Additional Diagnostic Results
TEST RESULTS
Ocular/retinal examination: Pinpoint retinal hemorrhages OU, no evidence of retinal detachment or hyphema.Urine protein creatinine ratio: 5.28 (normal < 0.5)
Heartworm antigen test: Negative
Serology for tick-borne diseases: Negative
Urine culture: Negative
Abdominal ultrasound: Cystic benign prostatic hyperplasia with concurrent paraprostatic cysts. Bilateral adrenomegaly. Renal findings consistent with bilateral chronic renal disease with cortical dystrophic mineralization. No evidence of renoliths or uroliths.
 Diagnosis
Diagnosis
You’re ready to form a diagnosis for Arco! Please select your answer to each question below.
What is your cardiac diagnosis for Arco?
Which of the following systemic findings is least likely to be related to Arco's severe systemic hypertension?
Click here to learn more about the stages of MMVD.
Treatment
You’re ready to form a treatment plan for Arco.
What treatment(s) would you recommend for Arco?
Follow Up
Please review Arco’s follow up
Arco’s castration surgery was postponed until his systemic condition had been stabilized. After a short hospitalization for fluid therapy, Arco’s creatinine stabilized at 4.9 mg/dL but his appetite was improved. At discharge, Arco’s blood pressure was improved at 178/102 (127) mmHg. Arco’s target systolic blood pressure is approximately 140 mmHg. An increase in the amlodipine dose may be needed if systolic blood pressure remains ≥ 160 mmHg 5-7 days post-initiation of antihypertensive therapy. Click here to view the updated ACVIM Systemic Hypertension Consensus Statement.
 Post Test - CE
Post Test - CE
Please answer the following questions.
What is normal systolic blood pressure in dogs (when measured noninvasively)?
What target organ change might be a result of severe systemic hypertension?
Which of the following tests can be used to investigate proteinuria?
A precordial thrill indicates that a heart murmur is at least what grade (on a standard grading scale of 1-6)?
Systemic hypertension may be associated with findings of mitral regurgitation and aortic regurgitation.
 RACE Certification
RACE Certification
RACE Certification
Fill out the following form in order to receive your certificate.