
Athena
 Case Background
Case Background
Name: Athena
Age: 6 years
Sex: Female
Breed: Doberman
Weight: 30 kg
Reason for Visit: Decreased appetite, cough and labored breathing
Medications: Amoxicillin 500mg: 1 capsule q 12hrs
Age: 6 years
Sex: Female
Breed: Doberman
Weight: 30 kg
Reason for Visit: Decreased appetite, cough and labored breathing
Medications: Amoxicillin 500mg: 1 capsule q 12hrs
 Clinical History
Clinical History
Please review Athena’s clinical history.
Attitude/Demeanor: Lethargic
Coughing: Coughing for two weeks
Abnormal Respirations: Increased respiratory effort over the last 2 days
Exercise Tolerance: Refusing to go on normal walks
Sleep Patterns: Prefers to lay in sternal recumbency which is atypical
Weight Change (loss or gain): None
Appetite: Has become very particular about food over the last 2 weeks
Usual Diet: Purina OM™, 4 cups per day
Vomiting: None
Diarrhea: None
Syncope: None
Change in urinary habits: None
Change in drinking habits: None
Other symptoms or signs: None
 Physical Exam - General
Physical Exam - General
Please review the results of Athena’s physical exam.
Body Condition: Good
Attitude: Quiet
Mobility | Gait: Ambulating normally
Posture: Standing or sternally recumbent
Hydration: Adequate
Body Temperature: 100.2 F
Arterial Pulse – rate, regularity, intensity: Weak, irregular pulses with a rate of 180/min with pulse deficits
Respiratory Effort: Increased respiratory effort.
Mucous Membranes – Color & CRT: Pale to pink / 3 seconds.
Jugular Venous Pulse & Pressure: No jugular distention
Abdominal Palpatation: Normal
Lymph Nodes: Normal.
Oral Cavity: Normal
Other Abnormalities: None
 Physical Exam - Auscultation
Physical Exam - Auscultation
Let’s auscult Athena’s heart & lungs.
WHAT DO YOU HEAR?
LISTEN TO ATHENA'S THORAX AND LUNGS. DO THEY SOUND NORMAL OR ABNORMAL?
 Physical Exam - Differential Diagnosis
Physical Exam - Differential Diagnosis
The following are potential diagnosis for you to consider at this time. Based on the history and the physical examination, please indicate the likelihood of each as:
- High (could explain most or all of the signs)
- Possible (less likely to explain most of the signs)
- Unlikely
DILATED CARDIOMYOPATHY
DEGENERATIVE VALVE DISEASE
PRIMARY RESPIRATORY DISEASE
Diagnostic Test Selection
NON-INVASIVE BLOOD PRESSURE
CBC WITH PLATELET COUNT
COAGULATION PROFILE
SERUM BIOCHEMICAL PROFILE (INCLUDES ELECTROLYTES)
URINALYSIS
SERUM THYROXINE (T4)
HEARTWORM ANTIGEN TEST
HEARTWORM ANTIBODY TEST
HEARTWORM MICROFILARIA TEST
NT-PROBNP
CARDIAC TROPONIN-I
BLOOD CULTURE
THORACOCENTESIS OR ABDOMINOCENTESIS FOR DIAGNOSIS OR THERAPY
THORACIC RADIOGRAPHS
ABDOMINAL RADIOGRAPHS
ECHOCARDIOGRAM WITH DOPPLER STUDIES
ABDOMINAL ULTRASOUND
ECG RHYTHM STRIP OR 6 LEAD ECG
AMBULATORY ECG - HOLTER ECG OR EVENT MONITOR
 Blood Pressure
Blood Pressure
Systolic Blood Pressure: 105 mmHg
Diastolic Blood Pressure: Not available for this case
Mean Blood Pressure: Not available for this case
Consensus Statements of the American College of Veterinary Internal Medicine (ACVIM) provides the veterinary community with up-to-date information on the pathophysiology, diagnosis, and treatment of clinically important animal diseases. In 2018, ACVIM published guidelines for the Identification, Evaluation, and Management of Systemic Hypertension in Dogs and Cats in the the Journal of Veterinary Internal Medicine.
Click here to view and download a PDF of the ACVIM Consensus Statement, Guidelines for the Identification, Evaluation, and Management of Systemic Hypertension in Dogs and Cats.
Diastolic Blood Pressure: Not available for this case
Mean Blood Pressure: Not available for this case
Consensus Statements of the American College of Veterinary Internal Medicine (ACVIM) provides the veterinary community with up-to-date information on the pathophysiology, diagnosis, and treatment of clinically important animal diseases. In 2018, ACVIM published guidelines for the Identification, Evaluation, and Management of Systemic Hypertension in Dogs and Cats in the the Journal of Veterinary Internal Medicine.
Click here to view and download a PDF of the ACVIM Consensus Statement, Guidelines for the Identification, Evaluation, and Management of Systemic Hypertension in Dogs and Cats.
 Radiographs
Radiographs
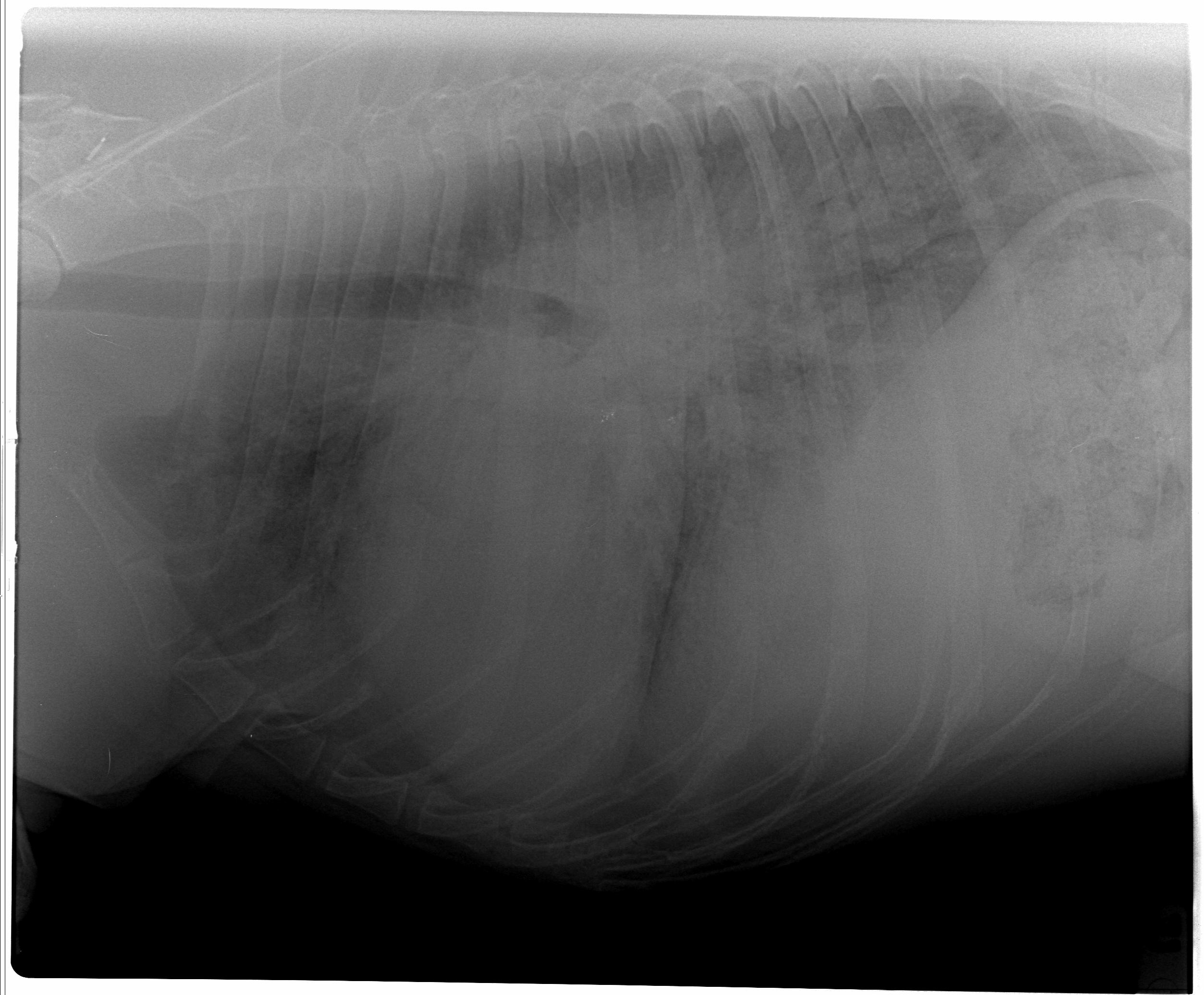
Please review Athena’s thoracic radiographs
Click here for Athena’s radiograph viewer (measure VHS and VLAS here) Click here for the right lateral viewAthena's right lateral view
Athena's ventral dorsal lateral view

WHAT IS THE VERTEBRAL HEART SIZE?
IS ATHENA'S HEART ENLARGED?
IF ATHENA’S HEART IS ENLARGED, WHICH CHAMBERS ARE INVOLVED?
IS THERE EVIDENCE OF CONGESTIVE HEART FAILURE PRESENT (PLEURAL EFFUSION OR PULMONARY EDEMA)?
 Clinical Labs
Clinical Labs
Please review Athena’s lab results
SERUM CHEMISTRIES
BUN: 24 mg/dL, Normal: 5 – 29 mg/dL
Creatinine: 1.7 mg/dL, Normal: 2.1 mg/dL
Sodium: 140 mmol/L, Normal:138 – 154 mmol/L
Potassium: 3.8 mEq/dL, Normal: 3.6 – 5.2 mEq/dL
Chloride: 115 mEq/dL, Normal: 105- 119 mEq/dL
ALT: 98 IU/dL, Normal: <75 IU/dL
ALP: 58 IU/dL, Normal: <100 IU/dL
Glucose: 140 IU/dL, Normal: 68 – 126 mg/dLHEARTWORM
Heartworm Test Results: NegativeURINALYSIS
Urinalysis – USG: 1.020
Urinalysis – Protein: Negative
Urinalysis – Biochemical: Negative
Urinalysis – Sediment Evaluation: NegativeCBC
White Blood Cells: 12,000/ul
Red Blood Cells: 41%
Platelets: 240,000/ul
 Echo
Echo
Please review the results of Athena’s echo.
Subjective – lesions of valves, myocardium, pericardial space: No valvular degeneration was seen. The left ventricular systolic function is subjectively reduced.
LV chamber size and thickness: There is severe left venticular eccentric dilation.
Left atrial size: The left atrium is moderately to severely enlarged.
LVIDd & LVIDs: Diastole (5.6 cm); Systole (5 cm).
LV shortening fraction: Left ventricular contractility is significantly reduced with a low fractional shortening of 11%.
RA, RV and Pulmonary Artery: Normal.
Effusions: No pleural or pericardial effusion.
Doppler results: There is moderate mitral valve regurgitation associated with geometric ventricular changes (dilation of the mitral valve annulus). Trivial tricuspid regurgitation.
Watch echo #1
 ECG
ECG
Please review Athena’s ECG.
Click to enlarge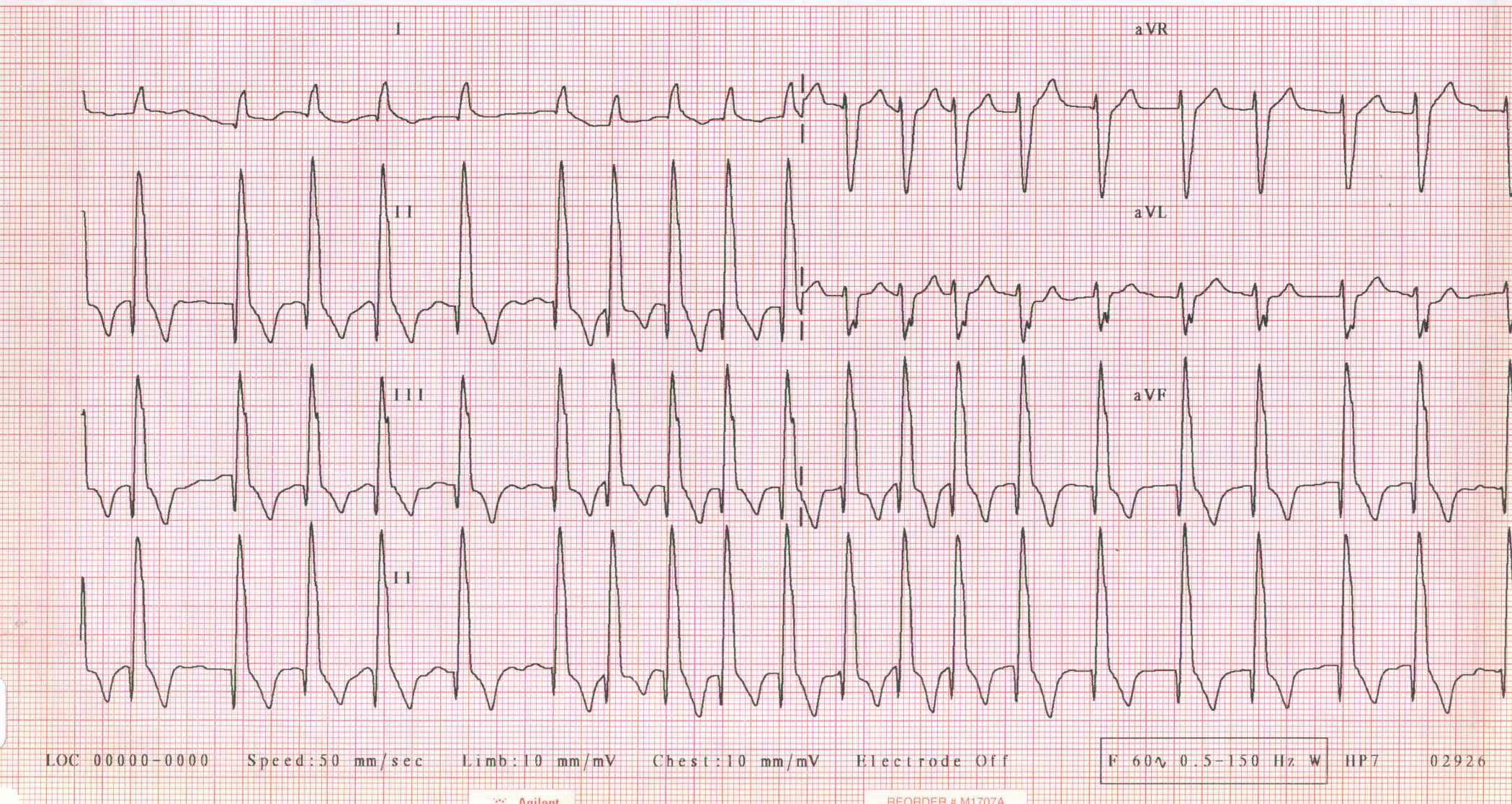
Athena's echocardiogram
RHYTHM DIAGNOSIS IS?
 Diagnosis
Diagnosis
Dilated Cardiomyopathy with left-sided congestive heart failure and atrial fibrillation: Stage C Dilated Cardiomyopathy
Dilated cardiomyopathy is a common form of heart disease that we see in large breed dogs. Reduced systolic function of the ventricular muscle results in volume overload and congestive heart failure. Arrhythmias are a common finding with dilated cardiomyopathy, and include ventricular tachyarrhythmias, and atrial fibrillation. Furosemide, enalapril, pimobendan have been prescribed to eliminate the cough and respiratory distress. The digoxin and diltiazem are being used to reduce the ventricular response rate to atrial fibrillation to prevent rate induced cardiomyopathy. Dilated cardiomyopathy is usually a progressive disease, with a poor long term prognosis. Dobermans can have a good quality of life for a number of months 3-12 months with appropriate management.
Treatment
Acute Treatment:
- Furosemide IV 3 mg/kg initial bolus
- Furosemide IV CRI 0.9ml/kg/hr for 4-8 hours until respiratory rate is <50 breaths/min
- Vetmedin 0.25 mg/kg PO q 8hrs
- Diltiazem (Regular) 2 mg/kg PO q8hr
Chronic Treatment: (To Go Home)
- Furosemide 2 mg/kg PO BID
- Enalapril 0.5 mg/kg PO BID
- Vetmedin 0.25 mg/kg PO BID
- Diltiazem XR 3 mg/kg PO BID
- Digoxin 0.003 mg/kg PO BID
Follow Up
Follow Up: A renal blood panel, an 8-hour post-pill serum digoxin concentration, ECG and thoracic radiographs should be performed in 5-7 days . The repeat radiographs are performed to ensure resolution of the pulmonary edema. An ECG is repeated to determine the need for additional rate control medication. The ventricular response rate goal would be an average of 135 bpm on Holter monitor, less than 140 bpm on a home ECG device or less than 160 on an in-hospital ECG in a calm patient. Thoracic radiographs, ECG, blood pressure and serum biochemistries should be repeated in 3-4 months to check for progression of congestive heart failure and additional rhythm disturbances, if no clinical signs have been noticed earlier.
7 Day Recheck: Athena was released after diagnostic tests and instituting oral therapy for CHF which included: Furosemide 2 mg/kg PO BID, enalapril 0.5 mg/kg PO BID, Vetmedin 0.25 mg/kg PO BID, and Diltiazem XR 3 mg/kg PO BID, Digoxin 0.003 mg/kg PO BID. She was re-examined 7 days later. The owners have not noticed any coughing or labored breathing since discharge from the hospital. The appetite was reduced for the first 3 days, and is near normal today. Athena ws assessed with a renal panel, 8-hour post-pill serum digoxin concentration, ECG and thoracic radiographs. Renal panel: BUN=37mg/dl; creatinine 1.8mg/dl; phosphorus and electrolytes are within normal limits. Serum digoxin concentration: 0.9ng/dl (sample was drawn 6-8 hours post-pill into a red top tube without a serum separator. Eight-hour post-pill (trough) concentrations between 0.8 and 1.3 ng/dl are ideal to help with rate control and prevent toxicity signs. ECG: Rhythm is still atrial fibrillation, but the rate has been effectively reduced to an average of 150 bpm on the in-hospital rhythm strip. Thoracic radiographs: Left-sided cardiomegaly with a tall, upright heart consistent with left ventricular enlargement with a moderate to severe caudodorsal bulge consistent with left atrial enlargement. However, the caudodorsal interstitial pattern noted previously is absent on today’s films, and there has been improvement in the pulmonary venous distention. An increase in the furosemide dose is not warranted.