
Sasha
 Case Background
Case Background
Name: Sasha
Age: 9.5 years old
Sex: Female
Breed: Cavalier King Charles Spaniel
Weight: 8.8 lbs (4.0 kg)
Reason for visit: Annual wellness evaluation
Medications: Heartworm prophylaxis, flea and tick prevention
Age: 9.5 years old
Sex: Female
Breed: Cavalier King Charles Spaniel
Weight: 8.8 lbs (4.0 kg)
Reason for visit: Annual wellness evaluation
Medications: Heartworm prophylaxis, flea and tick prevention
 Clinical History
Clinical History
Attitude/demeanor: Normal
Coughing: None
Respiration: Normal
Exercise tolerance: Normal
Sleep patterns: Normal
Weight change (loss or gain): None
Appetite: Normal
Usual diet: Royal Canin® adult small breed dried dog food
Vomiting: None
Diarrhea: None
Syncope: None
Change in urinary habits: None
Change in drinking habits: None
Living circumstances: Indoor with outdoor privileges under supervision, one other healthy dog
Coughing: None
Respiration: Normal
Exercise tolerance: Normal
Sleep patterns: Normal
Weight change (loss or gain): None
Appetite: Normal
Usual diet: Royal Canin® adult small breed dried dog food
Vomiting: None
Diarrhea: None
Syncope: None
Change in urinary habits: None
Change in drinking habits: None
Living circumstances: Indoor with outdoor privileges under supervision, one other healthy dog
 Physical Exam - General
Physical Exam - General
Body condition: 5/9
Attitude: Bright, alert, responsive
Mobility | gait: Normal
Posture: Normal
Hydration: Normal
Body temperature: 101.1 F
Arterial pulse – rate, regularity, intensity: 110 bpm, regular rhythm, normal amplitude
Rate & respiratory effort: 32 with normal effort
Mucous membranes – color & CRT: Light pink
Jugular venous pulse & pressure: Not examined
Abdominal palpatation: Normal
Lymph nodes: Normal
Oral cavity: Severe tartar and gingivitis
Other abnormalities: None
Attitude: Bright, alert, responsive
Mobility | gait: Normal
Posture: Normal
Hydration: Normal
Body temperature: 101.1 F
Arterial pulse – rate, regularity, intensity: 110 bpm, regular rhythm, normal amplitude
Rate & respiratory effort: 32 with normal effort
Mucous membranes – color & CRT: Light pink
Jugular venous pulse & pressure: Not examined
Abdominal palpatation: Normal
Lymph nodes: Normal
Oral cavity: Severe tartar and gingivitis
Other abnormalities: None
 Physical Exam - Auscultation
Physical Exam - Auscultation
Let’s ascult Sasha’s heart. (Recommend high-end headphones)
Palpitation of the chest wall overlying the heart (precordial palpitation) was normal. Sasha’s lung sounds are normal. These heart sounds were heard when the stethoscope was positioned over Sasha’s left apex. Listen to Sasha’s heartWhat is the grade of the systolic murmur?
 Physical Exam - Differential Diagnosis
Physical Exam - Differential Diagnosis
The following are potential diagnosis for you to consider at this time. Based on the history and the physical examination, please indicate the likelihood of each as:
- High (could explain most or all of the signs)
- Possible (less likely to explain most of the signs)
- Unlikely
MMVD with mitral regurgitation
Endocarditis with mitral regurgitation
DCM with mitral regurgitation
Hypertrophic cardiomyopathy with mitral regurgitation
Diagnostic Test Selection
Non-invasive blood pressure
CBC with platelet count
Serum biochemical profile (includes electrolytes)
Urinalysis
Heartworm antigen test
NT-PROBNP
Cardiac troponin-I
Thoracic radiographs
Echocardiogram
ECG rhythm strip or 6 lead ECG
 Blood Pressure
Blood Pressure
Systolic blood pressure: 134 mmHg (Doppler technique, forelimb)
Diastolic blood pressure: Not available for this case
Mean blood pressure: Not available for this case
Consensus Statements of the American College of Veterinary Internal Medicine (ACVIM) provides the veterinary community with up-to-date information on the pathophysiology, diagnosis, and treatment of clinically important animal diseases. In 2018, ACVIM published updated guidelines for the identification, evaluation, and management of systemic hypertension in dogs and cats in the the Journal of Veterinary Internal Medicine.
Click here to view and download a PDF of the ACVIM consensus statement, guidelines for the identification, evaluation, and management of systemic hypertension in dogs and cats.
Diastolic blood pressure: Not available for this case
Mean blood pressure: Not available for this case
Consensus Statements of the American College of Veterinary Internal Medicine (ACVIM) provides the veterinary community with up-to-date information on the pathophysiology, diagnosis, and treatment of clinically important animal diseases. In 2018, ACVIM published updated guidelines for the identification, evaluation, and management of systemic hypertension in dogs and cats in the the Journal of Veterinary Internal Medicine.
Click here to view and download a PDF of the ACVIM consensus statement, guidelines for the identification, evaluation, and management of systemic hypertension in dogs and cats.
 Radiography
Radiography
Please review Sasha’s thoracic radiographs.
Click here for Sasha’s radiograph viewer (measure VHS and VLAS here) View the ventral dorsal radiographSasha's annotated ventral dorsal lateral view

Sasha's right lateral view
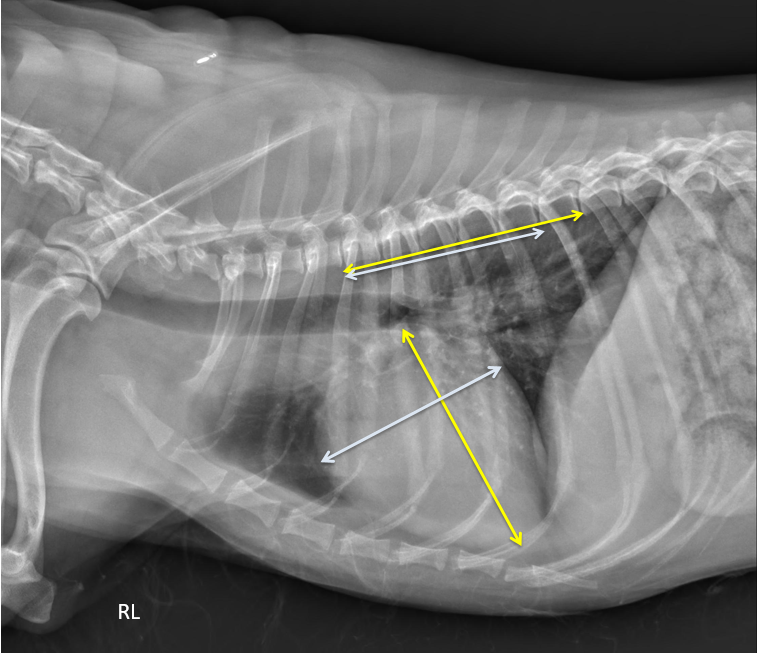
Sasha's annotated radiograph
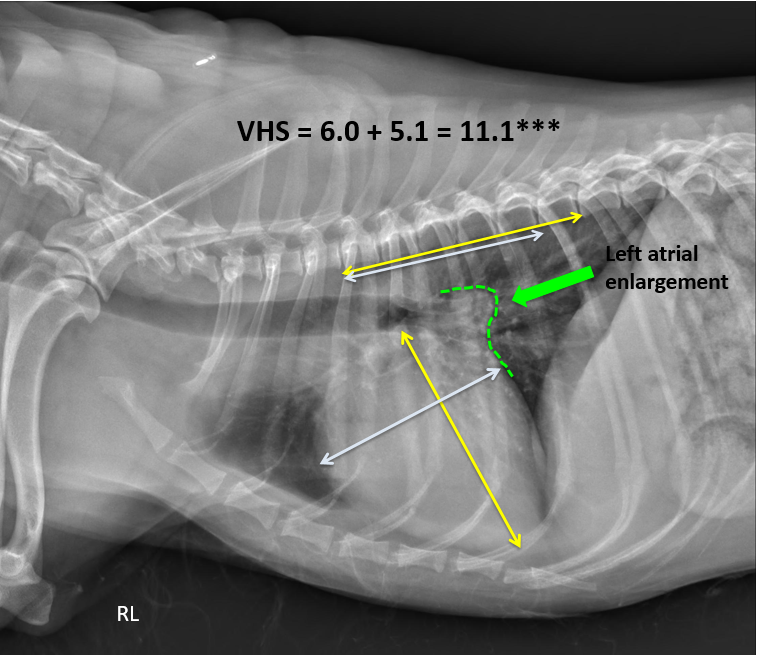
What is the vertebral heart size (VHS)?
Does this dog have left atrial enlargement?
Does this dog have evidence of congestive heart failure (pulmonary edema)?
What is the VLAS?
 Clinical Labs
Clinical Labs
SERUM CHEMISTRIES
BUN: 13 mg/dL, Normal: <30 mg/dLCreatinine: 0.88 mg/dL, Normal: <2.1 mg/dL
Sodium: 146 mEq/L, Normal:138 – 154 mEq/L
Potassium: 3.8 mEq/L, Normal: 3.6 – 5.2 mEq/L
Chloride: 113 mmol/L, Normal: 105 – 119 mEq/L
ALT: 55 IU/L, Normal: <75 IU/L
ALP: 28 IU/L, Normal: <100 IU/L
CBC
White blood cells: N/ARed blood cells: PCV = 42% Total Solids = 6.2 g/dl
Platelets: N/A
 Echocardiography
Echocardiography
Please review the results of Sasha’s echo.
Watch echo #1Watch echo #2
Watch echo #3
Watch echo #4
Subjective – lesions of valves, myocardium, pericardial space: The anterior and posterior leaflet were moderately thickened, with evidence of prolapse of the anterior valve leaflets. The cardiac rhythm was a normal sinus rhythm throughout the exam. No other abnormalities were noted.
LV chamber size and thickness: The left ventricular (LV) chamber size was normal in systole suggestive of preserved systolic function. The left ventricular chamber size was increased (dilated) in diastole with a calculated normalized index of 1.89.
Left atrial size: The left atrium (LA) was moderately dilated with a left atrial to aortic (Ao) ratio (2D, Swedish Method) = 1.6
LVIDd & LVIDs: LVIDd=3.59 cm (Index 1.89), LVIDs=2.04 cm (Index 1.03)
LV shortening fraction 43%
RA, RV and pulmonary artery: Right atrium (RA), right ventricle and main pulmonary artery were normal in size.
Effusions: None
Doppler results: Severe mitral regurgitation based on color Doppler imaging; turbulent flow fills the left atrium during systole. There was mild tricuspid regurgitation based on color Doppler the velocity was normal (2.6 m/sec). Normal velocity tricuspid regurgitation argues against pulmonary hypertension at this time.
 ECG
ECG
Given that the patient’s heart rate was regular on physical examination, the absence of pulse deficiets, and the absence clinical signs suggestive of an arrhythmia, this test was a low priority and not performed at this time. However, an ECG is sometimes recorded during an echocardiograpm. The simultaneous recording during echocardiography may be used to document normal sinus rhythm or detect arrhythmias that occur during the echocardiogram. In Sasha an ECG recorded durng the echocardiogram confirmed a normal sinus rythum.
 Referral
Referral
Consultation with a cardiologist or referral is never wrong and may be necessary if echocardiography is not locally available, or may occur at the owner’s request. In this case, referral was not required at this stage, Sasha’s owners declined this option. Click here to read the circulation article ABCDs of Cardiology Referral.
 Diagnosis & Treatment
Diagnosis & Treatment
You’re ready to form a diagnosis and treatment plan for Sasha! Please select your answer to each question below.
What is the most appropriate diagnosis?
What treatment(s) has/have been proven to prolong symptom-free survival and overall survival in dogs with stage B2 MMVD?
Follow Up
Follow-up treatment: Recheck of Stage B2 MMVD patients receiving pimobendan therapy is recommended approximately once every 6 months, or sooner if clinical signs suggestive of progressive heart disease develop (e.g. cough, increased sleeping respiration rate, exercise intolerance etc.). Typical recheck examinations include a thorough history and physical examination, thoracic radiographs and blood pressure assessment. Annual evaluation of routine blood values (especially renal values and electrolytes) is also recommended.
 Post Test - CE
Post Test - CE
To qualify for CE credit, please answer the following 5 questions.
The most common cause of a left apical systolic murmur in an older small breed dog Is:
The recommended treatment that has been proven to delay the onset of CHF and extend survival in dogs with stage B2 MMVD characterized by a combination of sufficient left atrial and left ventricular enlargement (LA:AO ≥ 1.6, normalized LVIDDN ≥ 1.7) is:
If an echocardiogram can not be performed in a dog suspected to have preclinical (stage B1 or B2) MMVD based on history, signalment and physical exam, but you have thoracic radiographs available for review. according to the CEG and the ACVI MMDV guidelines, what VHS can be used to support the initiation of pimobendan?
Concerning stage 2 MMVD, which of the following is/are correct? Owners should be instructed to
Each of the following diagnostic tests are considered low priority for a dog suspected to have preclinical (Stage B1 Or B2) MMVD based on history, signalment and physical exam.
 RACE Certification
RACE Certification
RACE Certification
Fill out the following form in order to receive your certificate.