
Skipper
 Case Background
Case Background
Name: Skipper
Age: 7 years
Sex: MN
Breed: Border Collie
Age: 7 years
Sex: MN
Breed: Border Collie
 Clinical History
Clinical History
Please review Skipper’s clinical history.
Skipper was presented for evaluation with a 2-week history of brief episodes of collapse with no loss of consciousness. He recovered to normal within 30 seconds. Thoracic auscultation revealed irregular heart rhythm, but no heart murmurs were detected. Other thoracic auscultation findings were normal. Pulses were strong but pulse deficits were detected.
 ECG
ECG
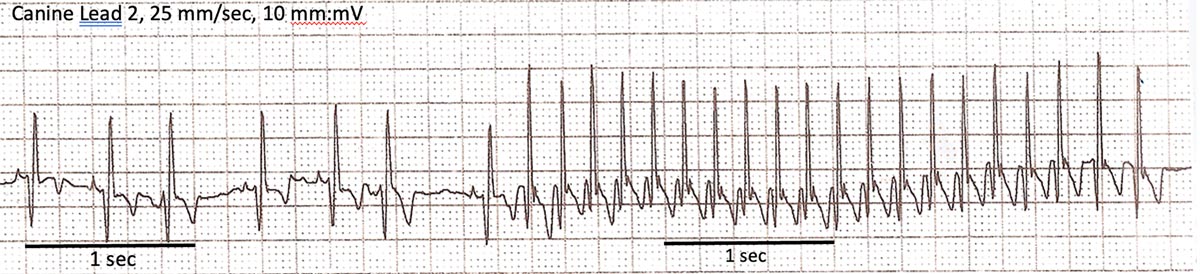
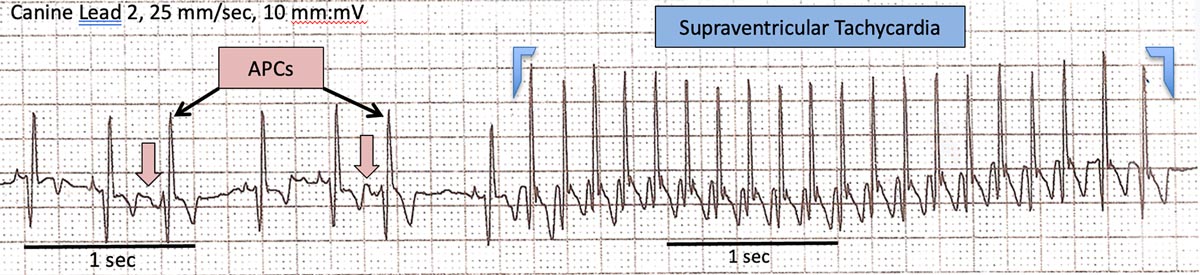
View Skipper’s electrocardiogram (the black bar represents one second)
{kind=link}
Which abnormalities are present on Skipper’s resting ECG?
{kind=link}
 Diagnosis & Treatment
Diagnosis & Treatment
Discussion:
Paroxysmal supraventricular tachycardia, especially at heart rates in excess of 300 bpm, may cause syncope or collapse when sudden rapid heart rate leads to a sudden drop in cardiac output. Although these arrhythmias are seldom associated with sudden death, treatment is required to maintain a reasonable quality of life in affected patients. Treatment/management: A full cardiac evaluation, including thoracic radiographs and echocardiography, is recommended to attempt to identify underlying cardiac diseases processes. Supraventricular tachycardias are frequently successfully controlled with diltiazem therapy. In an acute situation, this medication may be administered intravenously, but oral diltiazem is a reasonable choice of therapy both acutely and chronically. When significant underlying cardiac disease is present, diltiazem alone may not be sufficient to control the arrhythmia and digoxin therapy may be added to for additional antiarrhythmic effect. In some cases of SVT, catheter-guided electrical ablation of abnormal intracardiac pathways may be required to control the arrhythmia.