
Taz
 Case Background
Case Background
Name: Taz
Age: 11 years
Sex: Male, neutered
Breed: Shih Tzu (9kg)
Age: 11 years
Sex: Male, neutered
Breed: Shih Tzu (9kg)
 Clinical History − Visit #1
Clinical History − Visit #1
Please review Taz’s clinical history.
New cough that started 1 week ago. The cough was initially noted in the evening but now occurs frequently throughout the day and night. The resting respiratory rate at home is 34 (Normal is < 30). The heart rate is 160 and regular, and there is a grade 4/6 left apical systolic murmur. Lung sounds are increased bilaterally with soft inspiratory crackles in the caudal lung fields. The respiratory rate in the hospital is 46/min.
Click here to view the Circulations article on Resting Respiratory Rate.
 Radiographs − Visit #1
Radiographs − Visit #1
Please review Taz’s radiographs
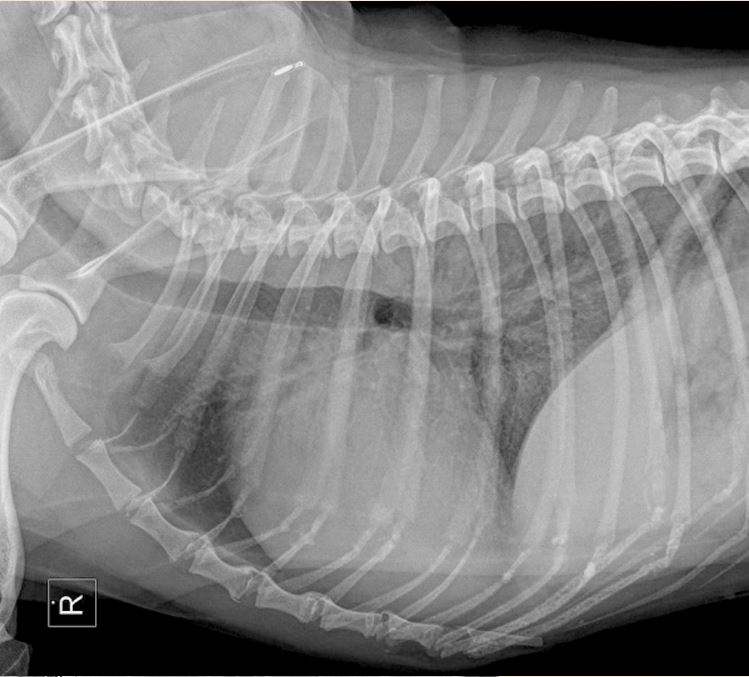
Click here for Taz’s radiograph viewer (measure VHS and VLAS here) View Taz's right lateral radiographTaz's right lateral radiograph
Taz's ventrodorsal radiograph

TECHNICAL DETAILS
Location of images: Thoracic radiographs obtained.
Views of images: Right lateral and ventrodorsal (VD)RADIOGRAPHIC FINDINGS
Technical issues: Good quality films, but no left lateral available.
Cardiac size including VHS: VHS=11.6 There is loss of the caudal waist on the right lateral consistent with moderate left atrial enlargement.
Other Findings: There is a mixed interstitial pattern in the caudodorsal lung fields that is moderate to severe. There is evidence of pulmonary venous distension, particularly in the caudal lung fields on the VD view.
 Diagnosis & Treatment − Visit #1
Diagnosis & Treatment − Visit #1
Radiographic Interpretation: Moderate generalized cardiomegaly with left atrial enlargement, pulmonary venous distension, and pulmonary infiltrate consistent with cardiogenic pulmonary edema. Findings are consistent with a diagnosis of Stage C MMVD.
Discussion: Dogs with stage C MMVD have current or previous signs of congestive heart failure. Click here for the ABCD Chart.
Treatment/Management: Initial treatment for CHF due to MMVD consists of furosemide and pimobendan. In this case they should be started immediately; furosemide at 2-3mg/kg IV or IM and pimobendan 0.25-0.3 mg/kg PO. An ACE inhibitor and spironolactone can be added at a later time. The parenteral dose of furosemide may need to be repeated q 1-2 hours until the dog appears stable. Additional supportive care may include oxygen supplementation and light sedation with butorphanol (0.2 mg/kg IV or IM) if the dog appears unduly stressed. Blood chemistries, a CBC, UA and blood pressure should be performed. Once the dog is able to be switched to oral furosemide, an ACEi should be added. Spironolactone can be added at a later time (1st or 2nd recheck). Dog should be rechecked in 10-14 days (rads and blood work), sooner if the cough and breathing rate do not improve. [Click here for the CEG Formulary: Cardiac Medications for Dogs]. The dog should be exercise restricted until stable (i.e. until after the first recheck in 10-14 days). No dietary changes should be recommended at this time.
Discussion: Dogs with stage C MMVD have current or previous signs of congestive heart failure. Click here for the ABCD Chart.
Treatment/Management: Initial treatment for CHF due to MMVD consists of furosemide and pimobendan. In this case they should be started immediately; furosemide at 2-3mg/kg IV or IM and pimobendan 0.25-0.3 mg/kg PO. An ACE inhibitor and spironolactone can be added at a later time. The parenteral dose of furosemide may need to be repeated q 1-2 hours until the dog appears stable. Additional supportive care may include oxygen supplementation and light sedation with butorphanol (0.2 mg/kg IV or IM) if the dog appears unduly stressed. Blood chemistries, a CBC, UA and blood pressure should be performed. Once the dog is able to be switched to oral furosemide, an ACEi should be added. Spironolactone can be added at a later time (1st or 2nd recheck). Dog should be rechecked in 10-14 days (rads and blood work), sooner if the cough and breathing rate do not improve. [Click here for the CEG Formulary: Cardiac Medications for Dogs]. The dog should be exercise restricted until stable (i.e. until after the first recheck in 10-14 days). No dietary changes should be recommended at this time.
Clinical History − Visit #2
Please review Taz’s follow-up.
Taz returns for a follow-up exam 12 days after the initial visit. His cough has resolved by 90%, and resting breathing rate is now 18/min. Heart rate is 130 and regular. The murmur is still present and unchanged in grade at 4/6. The lung sounds are normal and the respiratory rate in the hospital is 24/min.
Click here to view the Circulations article on Resting Respiratory Rate.
Radiographs − Visit #2
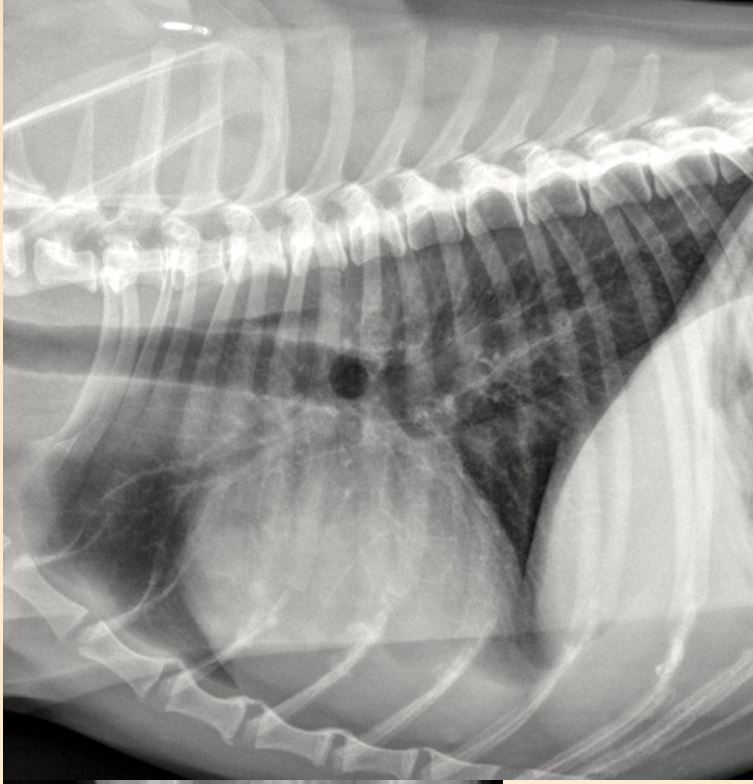
View Taz's right lateral radiograph
 View Taz's ventrodorsal radiograph
View Taz's ventrodorsal radiograph

Taz's right lateral radiograph
Taz's ventrodorsal radiograph
TECHNICAL DETAILS
Location of images: Thoracic radiographs obtained.
Views of images: Right lateral and ventrodorsal (VD)RADIOGRAPHIC FINDINGS
Technical issues: Good quality films.
Cardiac size including VHS: VHS=11.0 (reduced from previous exam by 0.6) There is loss of the caudal waist on the right lateral consistent with moderate left atrial enlargement.
Other Findings: Pulmonary venous distension is still visible in the left caudal lung field. No other significant findings are noted. (VD view).
Diagnosis & Treatment - Visit #2
Radiographic Interpretation: Persistent (although reduced from previous evaluation) moderate generalized cardiomegaly with left atrial enlargement. The lung parenchyma is within normal limits at this time consistent with resolution of the previously diagnosed congestive heart failure (cardiogenic pulmonary edema).
Discussion: The pulmonary edema has resolved and the cardiomegaly is persistent although somewhat reduced. Click here to view the CEG summary: The ABCDs of canine myxomaotous mitral valve disease.
Treatment/Management: This dog has responded optimally to initial heart failure therapy that included furosemide (2.2 mg/kg BID PO), pimobendan (0.28 mg/kg BID PO) and benazepil (0.4mg/kg BID PO). Blood chemistries were repeated and relatively unchanged (within normal limits), and the dog is clinically stable. There is no need to adjust the current medication doses and they should be continued chronically. Additionally, spironolactone at 1 mg/kg PO BID should be added as this may have a survival benefit long term. The owner should be encouraged to limit high sodium treats and start omega 3 supplementation. The dog should be allowed to exercise normally at this time (i.e. set their own pace). The next recheck should be 2-3 months, or sooner if clinical symptoms return (resting respiration rate is reproducibly >30/minute, the cough returns/worsens, or other signs of heart failure develop).
Discussion: The pulmonary edema has resolved and the cardiomegaly is persistent although somewhat reduced. Click here to view the CEG summary: The ABCDs of canine myxomaotous mitral valve disease.
Treatment/Management: This dog has responded optimally to initial heart failure therapy that included furosemide (2.2 mg/kg BID PO), pimobendan (0.28 mg/kg BID PO) and benazepil (0.4mg/kg BID PO). Blood chemistries were repeated and relatively unchanged (within normal limits), and the dog is clinically stable. There is no need to adjust the current medication doses and they should be continued chronically. Additionally, spironolactone at 1 mg/kg PO BID should be added as this may have a survival benefit long term. The owner should be encouraged to limit high sodium treats and start omega 3 supplementation. The dog should be allowed to exercise normally at this time (i.e. set their own pace). The next recheck should be 2-3 months, or sooner if clinical symptoms return (resting respiration rate is reproducibly >30/minute, the cough returns/worsens, or other signs of heart failure develop).