
Sophie
 Case Background
Case Background
Name: Sophie
Age: 7yr
Sex: Female, spayed
Breed: Cocker Spaniel
Age: 7yr
Sex: Female, spayed
Breed: Cocker Spaniel
 Clinical History
Clinical History
Please review Sophie’s clinical history.
Sophie presented for an annual wellness exam, and bradycardia was identified on physical examination
 ECG
ECG
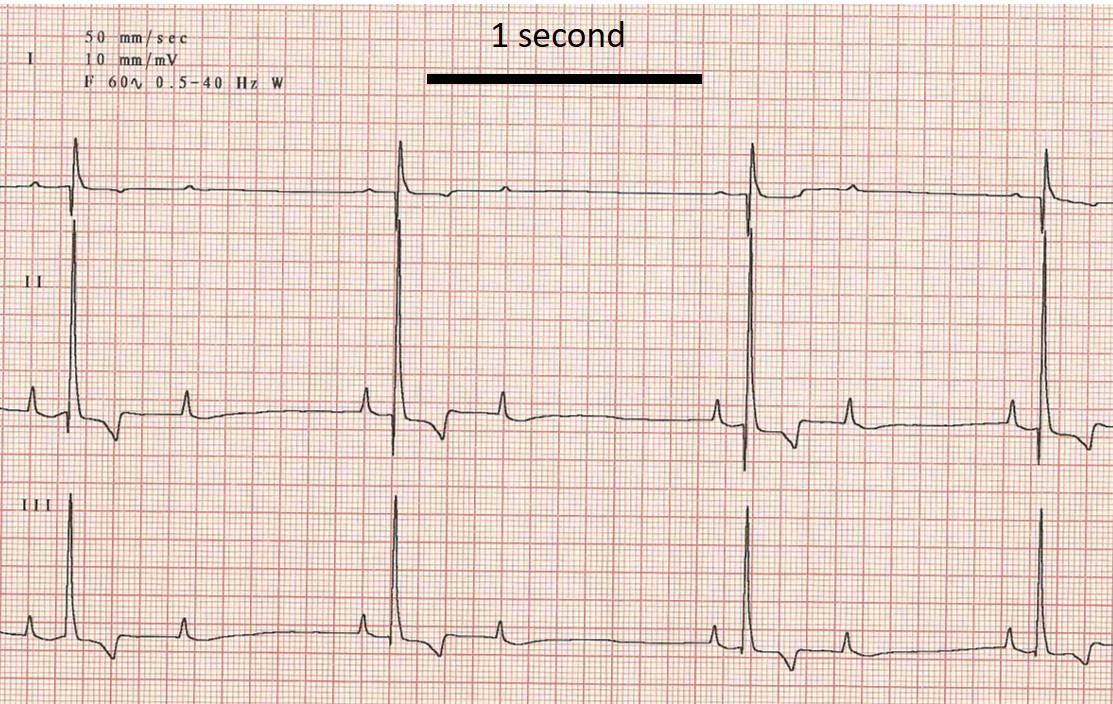
View Sophie’s electrocardiogram (the black bar represents one second)
{kind=link}
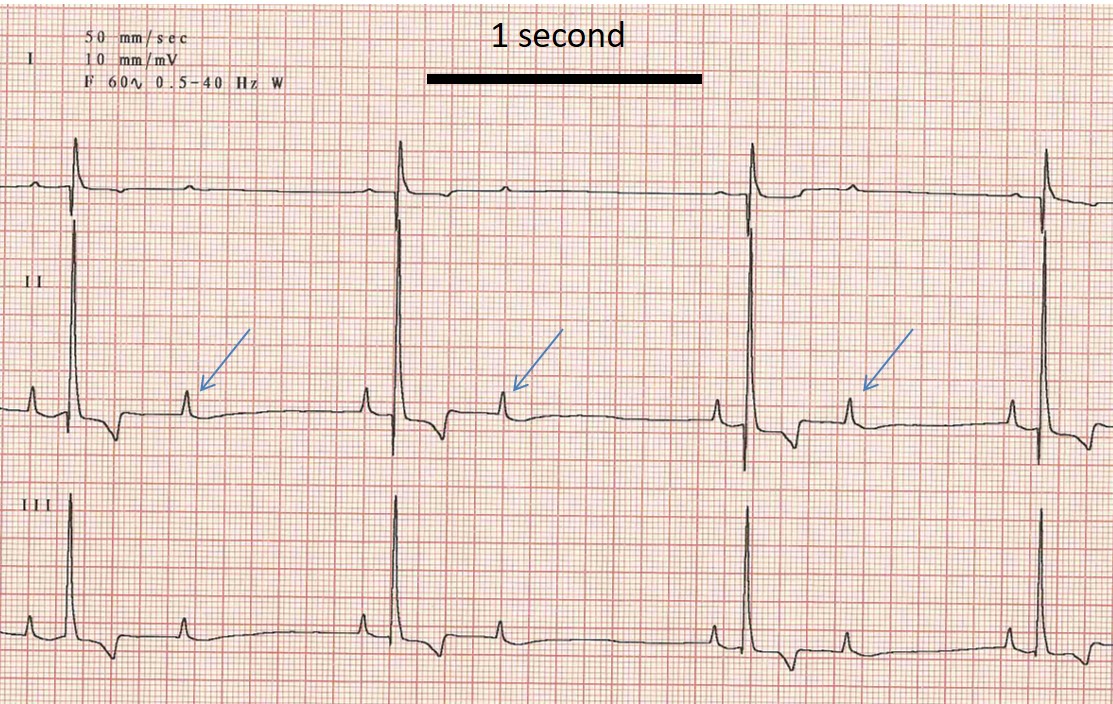
What abnormalities are present on this ECG?
{kind=link}
 Discussion & Treatment
Discussion & Treatment
Discussion: The presence of a second degree AV block is many times clinically silent, as in this case. The causes can be related to degeneration of the AV conduciton system which has the potential to progress to more severe forms of AV conduction disease (high grade second degree or 3rd degree block). In some cases, 2nd degree AV block can be a result of increased vagal tone, drugs (digoxin, alpha-2 agonists), or secondary to underlying metabolic disease. Treatment/management: When 2nd degree AV block is low grade and not associated with clinical signs, treatment is not always needed. Intermittent re-evaluation is necessary to monitor for progression to higher grades of block, which may result in clinical signs. The presence of a concurrent intra-ventricular conduction disturbance, such as a bundle branch block, implies more diffuse conduction disease. In many cases injectable atropine can be given to determine if a heart rate response is noted; a positive response is often seen in vagally-induced AV block. Most cases of persistent AV block should be evaluated by a cardiologist. The treatment of choice for high-grade second degree AV block and 3rd degree AV block is permanent pacemaker implantation.