
Sam
 Case Background
Case Background
Name: Sam
Age: 14 years
Sex: Male, neutered
Breed: Siamese cat
Age: 14 years
Sex: Male, neutered
Breed: Siamese cat
 Clinical History
Clinical History
Please review Sam’s clinical history.
The client believes he is slowing down a bit, but has attributed it to his older age. A slow heart rate was noted on examination and an ECG was therefore obtained.
 ECG
ECG
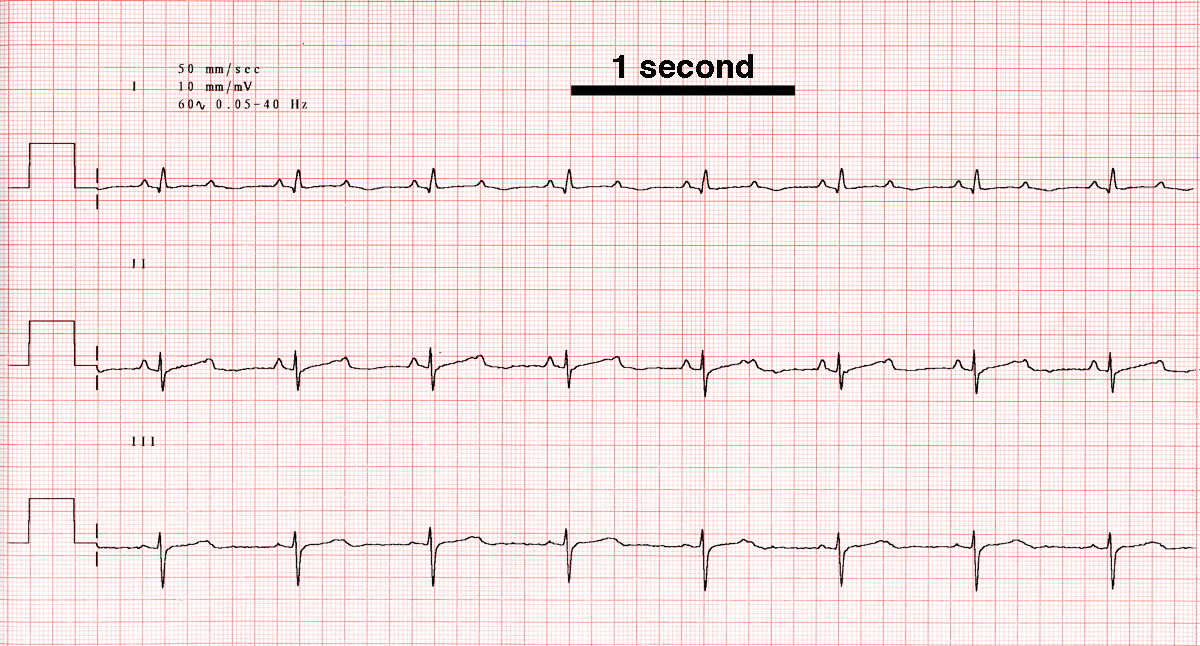
View Sam’s electrocardiogram (the black bar represents one second)
{kind=link}
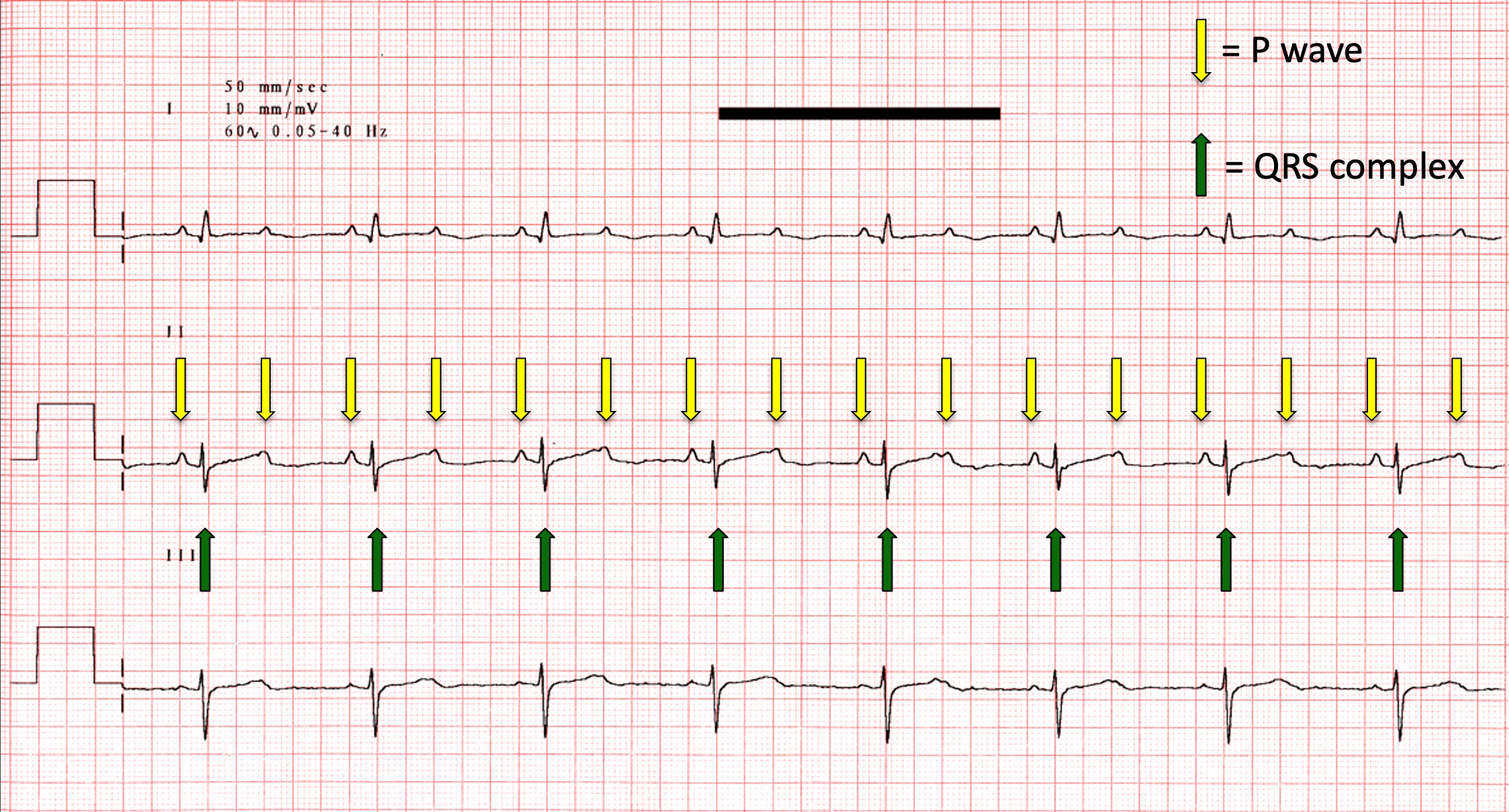
What abnormalities are present on this ECG?
{kind=link}
 Discussion & Treatment
Discussion & Treatment
Discussion:
Atrioventricular block and bundle branch blocks occur with degeneration and fibrosis of the conduction system, secondary to inflammation, or from tumor infiltration. In an older animal, age-related degeneration is the most common scenario. Rarely, echocardiography shows a tumor invading the interventricular septum and leading to AV block. Rare cases of myocarditis are also seen, often with unknown etiology, and are suspected based on a high cardiac troponin I in conjunction with an abnormal heart rhythm.
Treatment/management:
Persistent second degree AV block, such as this, often progresses to complete AV block and is typically resistant to medical therapy. Drugs that remove parasympathetic tone (atropine, glycopyrrolate, hyoscyamine) or increase sympathetic tone (dobutamine, terbutaline) may be attempted, but are rarely successful. Implantation of a pacemaker is often the only definitive therapy for symptomatic AV block. However, cats often have stable escape rhythms and may remain asymptomatic even when in complete (third degree) AV block. If the animal’s escape rhythm falters or clinical signs develop (syncope, weakness), pacing is generally recommended. In cats, transvenous pacemakers have been associated with caval obstruction and chylothorax; as such, epicardial pacing is more commonly pursued with the lead sutured to the heart and the generator implanted in the abdomen.