
Penny
 Case Background
Case Background
Name: Penny
Age: 7 years
Sex: Female, spayed
Breed: Feline, domestic long hair
Age: 7 years
Sex: Female, spayed
Breed: Feline, domestic long hair
 Clinical History
Clinical History
Please review Penny’s clinical history.
Presented for evaluation of tachypnea noted by the referring veterinarian. The cat has a poor appetite and is less active. The referring DVM obtained two view radiographs (see radiographs in radiograph tab to the right). Physical examination also indicated prominent jugular veins and a possible gallop sound.
 Radiographs
Radiographs
View Penny's right lateral radiograph
 View Penny's ventrodorsal radiograph
View Penny's ventrodorsal radiograph
 Click here for Penny’s radiograph viewer
Click here for Penny’s radiograph viewer
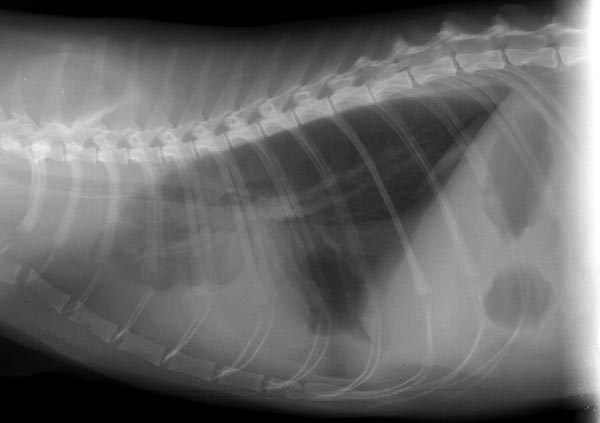
Penny's right lateral radiograph
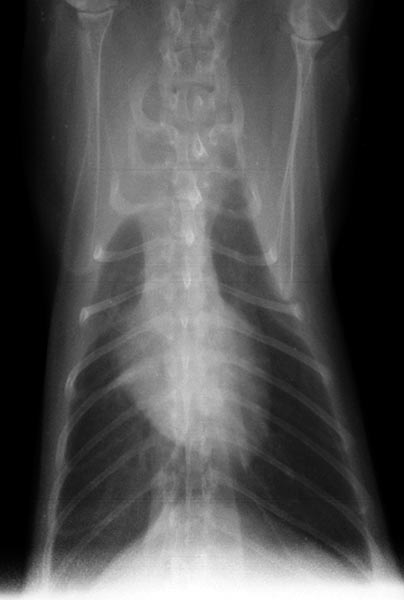
Penny's ventrodorsal radiograph
Radiographic findings Technical issues: None, other than a left lateral view was not obtained The heart is subjectively enlarged, appearing tall on the lateral view, but is obscured in part by fluid density and cannot be completely assessed. Careful inspection of the caudal lung fields on the VD shows a retraction of the borders, indicative of pleural effusion bilaterally. Pleural effusion is also evident on the lateral view. There is border effacement (silhouetting) of the cardiac and diaphragmatic shadows with a widened cranial mediastinum. The cranial lobes are displaced caudally (see the lateral view), especially the right cranial lobe (see the VD view). Additionally, on the lateral view, there is the typical scalloped appearance of a fluid/air interface in the ventral 1/3 of the thorax. The caudal vena cava appears dilated, though somewhat obscured by pleural or mediastinal fluid. Pulmonary vessels appear normal in size. The diaphragm appears intact. On the lateral view the caudal blood vessel margins are clear, suggesting there is no significant intra-pulmonary density. Radiographic interpretation: Pleural effusion in cats is a common problem and can be caused by congestive heart failure, neoplasia (lymphoma, metastatic disease), chylothorax, FIP, pyothorax, and hemithorax among other causes. Discussion: The main findings are possible cardiomegaly, a large caudal vena cava, and bilateral pleural effusion without evidence of trauma (no subcutaneous air, no rib fractures, and an intact diaphragm). Based on these findings congestive heart failure must be considered as well as other causes of pleural effusion such as chylothrorax (that also can be due to CHF), pyothorax, hemothorax, and modified transudates related to neoplasia. Thoracocentesis with cytology could be useful diagnostically. However, the exam of choice would likely be an ultrasound/ echocardiogram of the thorax.This could help exclude a mediastinal mass (lymphoma, thymoma) and evaluate the heart size and function. As pleural effusion in a cat is always serious, a complete workup is generally indicated, including blood and urine tests. FeLV and FIV status should also be documented.
 Diagnosis & Treatment
Diagnosis & Treatment
Diagnosis: The mediastinum in this cat was normal on ultrasound and echocardiography showed marked dilation of the right atrium and moderate dilation of the right ventricle. The tricuspid and pulmonic valves were normal and there was no atrial septal defect or dilation of the pulmonary arteries to suggest pulmonary hypertension. The clinical diagnosis was right ventricular cardiomyopathy (arrhythmogenic right ventricular cardiomyopathy) with congestive heart failure. This diagnosis is supported by the jugular distension and dilated caudal vena cava. Cytology of the fluid showed a modified transudate. Treatment/management: The cat was treated for congestive heart failure with furosemide, enalapril, and extra-label pimobendan and did improve on this therapy.